You might also like
- Ocular Emergencies Red EyeDocument25 pagesOcular Emergencies Red EyeolakasturiNo ratings yet
- Ocular Emergencies 2017Document18 pagesOcular Emergencies 2017Sebastian BarreraNo ratings yet
- Iritis 8Document14 pagesIritis 8Alvis KurniawanNo ratings yet
- Redeye Mini Case 2017 Tutor's Guide PDFDocument9 pagesRedeye Mini Case 2017 Tutor's Guide PDFJoanna GarciaNo ratings yet
- Emergencias Oculares Affp 13Document5 pagesEmergencias Oculares Affp 13Mario Villarreal LascarroNo ratings yet
- Red EyeDocument32 pagesRed EyeVitor ParenteNo ratings yet
- Optho HXDocument5 pagesOptho HXChris KingNo ratings yet
- The Pediatric Red Eye: Melissa M. Wong,, William AnningerDocument1 pageThe Pediatric Red Eye: Melissa M. Wong,, William AnningeredupomarNo ratings yet
- Another JurnalDocument4 pagesAnother JurnalReskyAmeliaHRNo ratings yet
- Evaluation of The Red EyeDocument6 pagesEvaluation of The Red EyeAileen Denisse Aquino VizaNo ratings yet
- Disturbance in Sensory PerceptionDocument48 pagesDisturbance in Sensory PerceptionKristine Louise JavierNo ratings yet
- The Red Eye: Evaluation and ManagementDocument42 pagesThe Red Eye: Evaluation and Managementmatheus mouraNo ratings yet
- Evaluation of The Painful EyeDocument9 pagesEvaluation of The Painful EyeMuthia Farah AshmaNo ratings yet
- Ruptur BulbiDocument5 pagesRuptur BulbiseptrealtiNo ratings yet
- Ophthalmology Referral Guidelines: Document IDDocument28 pagesOphthalmology Referral Guidelines: Document IDBambang AdiNo ratings yet
- K.15 Ophtalmologic EmergenciesDocument35 pagesK.15 Ophtalmologic EmergenciesZikri Putra Lan Lubis100% (1)
- Tgs ReferatDocument44 pagesTgs ReferatlieNo ratings yet
- Silo - Tips - How To Take An Ophthalmic HistoryDocument5 pagesSilo - Tips - How To Take An Ophthalmic HistorySumon SarkarNo ratings yet
- Protrusion OjoDocument16 pagesProtrusion OjoAntonio ReaNo ratings yet
- Anatomi Dan Fisiologi KorneaDocument133 pagesAnatomi Dan Fisiologi KorneaAriyanie NurtaniaNo ratings yet
- Eye Trauma: Brief IntroductionDocument16 pagesEye Trauma: Brief IntroductionOchi D. GreenNo ratings yet
- Choi Eye Emergencies 9.16Document3 pagesChoi Eye Emergencies 9.16pascutaNo ratings yet
- Cataract PTDocument9 pagesCataract PTPreeti SharmaNo ratings yet
- Cataract PTDocument9 pagesCataract PTpreeti sharmaNo ratings yet
- Vernal Keratoconjunctivitis: Why Is Allergic Eye Disease A Problem For Eye Workers?Document3 pagesVernal Keratoconjunctivitis: Why Is Allergic Eye Disease A Problem For Eye Workers?darendraabimayuNo ratings yet
- Ocular Emergencies: AssessmentDocument7 pagesOcular Emergencies: AssessmentradhikasreedharNo ratings yet
- LTM SenseDocument6 pagesLTM SenseNabilla MerdikaNo ratings yet
- Homeo Eye DiseaseDocument15 pagesHomeo Eye DiseaseAlbena Trifonova100% (3)
- Blepharitis Disease and Its ManagementDocument7 pagesBlepharitis Disease and Its Managementνικος νικουNo ratings yet
- Standard Treatment Guidelines Opthalmology Author Dr. Venkatesh PrajnaDocument146 pagesStandard Treatment Guidelines Opthalmology Author Dr. Venkatesh PrajnaAriana BulaiNo ratings yet
- Health Assessment - EYES ReviewerDocument6 pagesHealth Assessment - EYES ReviewerAnna Juliana SitoNo ratings yet
- Eye DiseasesDocument8 pagesEye DiseasesCeline de HaanNo ratings yet
- Group 3 CC: Girl Rubbing Her R Eye After TraumaDocument4 pagesGroup 3 CC: Girl Rubbing Her R Eye After TraumaNoemi Rebollos SuladayNo ratings yet
- Ocular EmergenciesDocument26 pagesOcular EmergenciesYukianesa100% (1)
- Causes of Eye DischargeDocument4 pagesCauses of Eye Dischargeabed alawiNo ratings yet
- Glaukoma Case ReportDocument9 pagesGlaukoma Case ReportHIstoryNo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Downloadophthalmology Cases All Team PDF PDF Free - HTMLDocument23 pagesDownloadophthalmology Cases All Team PDF PDF Free - HTMLDương Yến TrânNo ratings yet
- Guidelines For The Management of Corneal Ulcer WHODocument36 pagesGuidelines For The Management of Corneal Ulcer WHOichalledhaNo ratings yet
- Traumatic Hyphema: A Teaching Case Report: Priscilla Lenihan, OD Dorothy Hitchmoth, OD, FAAODocument9 pagesTraumatic Hyphema: A Teaching Case Report: Priscilla Lenihan, OD Dorothy Hitchmoth, OD, FAAOMarshaNo ratings yet
- Red Eye CheckDocument3 pagesRed Eye CheckkrishnaNo ratings yet
- Ophthalmology Important QuestionsDocument9 pagesOphthalmology Important QuestionsGhaidaa SadeqNo ratings yet
- Activity7 (Sympathetic Ophthalmia)Document4 pagesActivity7 (Sympathetic Ophthalmia)Gabbii CincoNo ratings yet
- Acknowledgement: Aniridia Associated With Congenital Aphakia and Secondary GlaucomaDocument3 pagesAcknowledgement: Aniridia Associated With Congenital Aphakia and Secondary GlaucomaNisrina FarihaNo ratings yet
- Eye Osce 3Document39 pagesEye Osce 3epic sound everNo ratings yet
- Manual of Eye Emergencies Diagnosis and ManagementDocument221 pagesManual of Eye Emergencies Diagnosis and ManagementPhilip McNelson100% (2)
- Common Eye DiseasesDocument54 pagesCommon Eye Diseaseskyro draxNo ratings yet
- Mentahan PPT Lapsus DR BasDocument20 pagesMentahan PPT Lapsus DR BasArlinda Silva PrameswariNo ratings yet
- 100255-Article Text-1482-2-10-20220311Document6 pages100255-Article Text-1482-2-10-20220311Fachry RahmanNo ratings yet
- Contact Lens Complications and ManagementDocument10 pagesContact Lens Complications and Managementstrawberry8832850% (2)
- A Review of Optic NeuritisDocument5 pagesA Review of Optic NeuritissatrianiNo ratings yet
- Blurred VisionDocument7 pagesBlurred VisionRichi CiriacoNo ratings yet
- NCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDocument18 pagesNCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDiego DumauaNo ratings yet
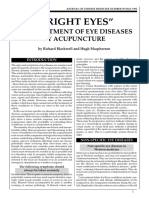
- Bright Eyes - The Treatment of Eye Diseases by AcupucntureDocument8 pagesBright Eyes - The Treatment of Eye Diseases by AcupucntureElizabeth Durkee Neil100% (1)
- Red Eye Clinical Presentation: History and Physical ExaminationDocument11 pagesRed Eye Clinical Presentation: History and Physical ExaminationLaiba KhanNo ratings yet
- Policy Statement Red Reflex Examination in Neonates, Infants and ChildrenDocument6 pagesPolicy Statement Red Reflex Examination in Neonates, Infants and ChildrenLore Sirpa MNo ratings yet
- CD 2Document14 pagesCD 2Amira AlmutairiNo ratings yet
- Clinical Symptoms: Go ToDocument2 pagesClinical Symptoms: Go ToMaria Dominga Baylon DiazNo ratings yet
- Ophthalmology PDFDocument28 pagesOphthalmology PDFKukuh Rizwido PrasetyoNo ratings yet
- Baseline Leukocyte Count and Acute CoronaryDocument5 pagesBaseline Leukocyte Count and Acute CoronaryMuhammad Dadan KurniawanNo ratings yet
- Laboratory Assesment of Thyroid Function PMC2003Document14 pagesLaboratory Assesment of Thyroid Function PMC2003Muhammad Dadan KurniawanNo ratings yet
- Blood Glucose and Its PrognosticDocument7 pagesBlood Glucose and Its PrognosticMuhammad Dadan KurniawanNo ratings yet
- Acmg Practice Guideline Genetic Evaluation Of.13Document6 pagesAcmg Practice Guideline Genetic Evaluation Of.13Muhammad Dadan Kurniawan100% (1)
- Management of Hyperglycaemia in Acute Coronary Syndrome PDFDocument8 pagesManagement of Hyperglycaemia in Acute Coronary Syndrome PDFMuhammad Dadan KurniawanNo ratings yet
- Journal Reading KolelithiasisDocument3 pagesJournal Reading KolelithiasisMuhammad Dadan KurniawanNo ratings yet
- DsDocument3 pagesDsMuhammad Dadan KurniawanNo ratings yet
- Prognostic Value of White Blood Cell Count in Acute Myocardial Infarction - Long-Term Mortality - Revista Española de Cardiología (English Version)Document3 pagesPrognostic Value of White Blood Cell Count in Acute Myocardial Infarction - Long-Term Mortality - Revista Española de Cardiología (English Version)Muhammad Dadan KurniawanNo ratings yet
- Neutrophilia Predicts Death and HeartDocument20 pagesNeutrophilia Predicts Death and HeartMuhammad Dadan KurniawanNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptMuhammad Dadan KurniawanNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Document1 pageP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Muhammad Dadan KurniawanNo ratings yet
- SCL-90-R & BsiDocument14 pagesSCL-90-R & Bsidrmss0% (1)
- Leukocytosis and Ischemic VascularDocument36 pagesLeukocytosis and Ischemic VascularMuhammad Dadan KurniawanNo ratings yet
- Elevated Cardiac Troponin I in Sepsis and Septic Shock 2010Document5 pagesElevated Cardiac Troponin I in Sepsis and Septic Shock 2010Muhammad Dadan KurniawanNo ratings yet
- Bakhbakhi Et AlDocument7 pagesBakhbakhi Et AlMuhammad Dadan KurniawanNo ratings yet
- FrostbiteDocument8 pagesFrostbiteMuhammad Dadan KurniawanNo ratings yet
- FrostbiteDocument8 pagesFrostbiteMuhammad Dadan KurniawanNo ratings yet
- Survey 40 Years Substitution MethadoneDocument14 pagesSurvey 40 Years Substitution MethadoneMuhammad Dadan KurniawanNo ratings yet
- Psychosis GuidelinesDocument26 pagesPsychosis GuidelinesMuhammad Dadan KurniawanNo ratings yet
- Cardiovascular DisordersDocument7 pagesCardiovascular Disordersapi-3712326100% (3)
- Scl-90-R Symptom Checklist-90-Revised Interpretive Report: Leonard R. Derogatis, PHDDocument5 pagesScl-90-R Symptom Checklist-90-Revised Interpretive Report: Leonard R. Derogatis, PHDMuhammad Dadan KurniawanNo ratings yet
- About Hiv and Its TreatmentDocument55 pagesAbout Hiv and Its TreatmentFiqih AdhyaksafitriNo ratings yet
- Drug Use and GenderDocument4 pagesDrug Use and GenderMuhammad Dadan KurniawanNo ratings yet
- Antibiotic Management of SuspectedDocument10 pagesAntibiotic Management of SuspectedMuhammad Dadan KurniawanNo ratings yet
- M 717Document16 pagesM 717Muhammad Dadan KurniawanNo ratings yet
- Methadone Maintenance TherapyDocument5 pagesMethadone Maintenance TherapyMuhammad Dadan KurniawanNo ratings yet
- Correlations Between Self-Reported Symptoms and PsychosocialDocument5 pagesCorrelations Between Self-Reported Symptoms and PsychosocialMuhammad Dadan KurniawanNo ratings yet
- JHBBDocument2 pagesJHBBMuhammad Dadan KurniawanNo ratings yet
- JHBBDocument2 pagesJHBBMuhammad Dadan KurniawanNo ratings yet
- JHBBDocument2 pagesJHBBMuhammad Dadan KurniawanNo ratings yet
- Lab ResultDocument1 pageLab ResultTanvir HamimNo ratings yet
- Transcultural NursingDocument3 pagesTranscultural NursingregineNo ratings yet
- Tired 2. Motivated 3. Excited 4. Scared 5. Angry 6. Happy 7. Disappointed 8. Bored 9. Delighted 10.sadDocument11 pagesTired 2. Motivated 3. Excited 4. Scared 5. Angry 6. Happy 7. Disappointed 8. Bored 9. Delighted 10.sadAnita Zarza BandaNo ratings yet
- Brochure Kerala Happiness Festival 2021 (July 27, 5.45-8.45 PM, Digital)Document5 pagesBrochure Kerala Happiness Festival 2021 (July 27, 5.45-8.45 PM, Digital)Rajesh PillaniaNo ratings yet
- ĐỀ THI THỬ 2021 - THPT QUẢNG XƯƠNG - THANH HOÁDocument11 pagesĐỀ THI THỬ 2021 - THPT QUẢNG XƯƠNG - THANH HOÁNguyen NhanNo ratings yet
- Model Health Officer Job DescriptionDocument4 pagesModel Health Officer Job DescriptionEsamNo ratings yet
- PHSA Blood and Body Fluid Exposure Control PlanDocument4 pagesPHSA Blood and Body Fluid Exposure Control PlanAndyDunnNo ratings yet
- Organizing Is Good For Mental HealthDocument2 pagesOrganizing Is Good For Mental Healthamos wabwileNo ratings yet
- Ethics Case StudyDocument4 pagesEthics Case StudycasscactusNo ratings yet
- Kelompok Tugas Farmakoterapi LanjutanDocument2 pagesKelompok Tugas Farmakoterapi LanjutanWahyu Mafrudin .ANo ratings yet
- Lecture - Maternal Health Concerns (Part 1)Document1 pageLecture - Maternal Health Concerns (Part 1)Rovilyn DizonNo ratings yet
- Agen InhalasiDocument22 pagesAgen InhalasiMuhammad Baihaqi SiddiqNo ratings yet
- Nursing SeatmatrixDocument8 pagesNursing SeatmatrixKanza KaleemNo ratings yet
- J. William Lloyd - The Karezza Method PDFDocument32 pagesJ. William Lloyd - The Karezza Method PDFmmm100% (1)
- Rle Opd (Case Study)Document13 pagesRle Opd (Case Study)Quintin MangaoangNo ratings yet
- Birla Institute of Technology & Science, Pilani Work Integrated Learning Programmes DigitalDocument10 pagesBirla Institute of Technology & Science, Pilani Work Integrated Learning Programmes DigitalAAKNo ratings yet
- SSC CGL Mains 2023 (4 Mock Test)Document23 pagesSSC CGL Mains 2023 (4 Mock Test)M thebluegirlNo ratings yet
- Practical Research 2 Module 4 Q1Document4 pagesPractical Research 2 Module 4 Q1Black CombatNo ratings yet
- RCC 3.15Document18 pagesRCC 3.15Hayley Rose100% (1)
- Research Journal The Pendulum 2018 CompressedDocument144 pagesResearch Journal The Pendulum 2018 Compressedgladys damNo ratings yet
- Hbo Midterm Exam Reviewer PDFDocument11 pagesHbo Midterm Exam Reviewer PDFMary Ellen LuceñaNo ratings yet
- EEF Active Ingredients SummaryDocument7 pagesEEF Active Ingredients SummarysoheiljavidNo ratings yet
- Revised ToR For The Consultancy Firm 01.09.2023Document14 pagesRevised ToR For The Consultancy Firm 01.09.2023Muvindu JayasingheNo ratings yet
- Kel 3 A Midwifery Model of Care ForDocument13 pagesKel 3 A Midwifery Model of Care ForWawa KurniaNo ratings yet
- US V RodgersDocument12 pagesUS V RodgersMelissa BoughtonNo ratings yet
- ATLS Post TestDocument1 pageATLS Post Testanon_57896987836% (56)
- Archipelago Food & Beverages Inc.: Site Master FileDocument14 pagesArchipelago Food & Beverages Inc.: Site Master FileQuality Assurace TeamNo ratings yet
- Lakewood Police Department Return To Work Decision MatrixDocument1 pageLakewood Police Department Return To Work Decision MatrixMichael_Roberts2019No ratings yet
- Public Health Nursing Population Centered Health Care in The Community Stanhope 8th Edition Test BankDocument13 pagesPublic Health Nursing Population Centered Health Care in The Community Stanhope 8th Edition Test Bankdominiecabasfsa28100% (45)
- Maharashtra University of Health Sciences, Nashik: Direction No. 8 of 1999 SubjectDocument38 pagesMaharashtra University of Health Sciences, Nashik: Direction No. 8 of 1999 SubjectSanthosh.S.UNo ratings yet