You might also like
- Review of Respiratory PhysiologyDocument46 pagesReview of Respiratory Physiologylovelyc95No ratings yet
- Interpret The Abgs in A Stepwise Manner:: Reference ReferenceDocument6 pagesInterpret The Abgs in A Stepwise Manner:: Reference ReferenceYogeshRavalNo ratings yet
- Interpretation of Arterial Blood Gases and Acid-Base DisordersDocument44 pagesInterpretation of Arterial Blood Gases and Acid-Base DisordersSuren VishvanathNo ratings yet
- Med Lecture - Causes of HypoxemiaDocument6 pagesMed Lecture - Causes of HypoxemiaZoherNBezantiNo ratings yet
- ABG Made EasyDocument9 pagesABG Made EasyDrShruthi PradeepNo ratings yet
- Translateturn Off Instant TranslationDocument38 pagesTranslateturn Off Instant TranslationListaNo ratings yet
- ABG InterpretationDocument38 pagesABG Interpretationmahmod omerNo ratings yet
- AbgDocument66 pagesAbgindyaphdNo ratings yet
- Arterial Blood Gas AnalysisDocument23 pagesArterial Blood Gas AnalysisVartika SainiNo ratings yet
- Gas ExchangeDocument15 pagesGas ExchangeOsolemio Mer100% (1)
- Interpretation of Blood Gas Reports - Made Easy: Dr. A K Sethi's EORCAPS-2010, DelhiDocument0 pagesInterpretation of Blood Gas Reports - Made Easy: Dr. A K Sethi's EORCAPS-2010, DelhiPrabhakar KumarNo ratings yet
- Common Causes of HypoxemiaDocument6 pagesCommon Causes of HypoxemiaSamantha LuiNo ratings yet
- Measures of Oxygenation and Mechanisms of Hypoxemia - UpToDateDocument11 pagesMeasures of Oxygenation and Mechanisms of Hypoxemia - UpToDateraniakusmantoNo ratings yet
- Interpreting Arterial Blood Gas Results: Nicholas J Cowley, Andrew Owen, Julian F BionDocument4 pagesInterpreting Arterial Blood Gas Results: Nicholas J Cowley, Andrew Owen, Julian F BionNayem Hossain HemuNo ratings yet
- Oxygen TransportDocument40 pagesOxygen TransportMike MayerNo ratings yet
- ABGDocument16 pagesABGKesavanVeeraNo ratings yet
- Metabolic Rate and Alveolar VentilationDocument9 pagesMetabolic Rate and Alveolar VentilationSimran SukhijaNo ratings yet
- Interpretasi Agd Juni 2020Document34 pagesInterpretasi Agd Juni 2020Christiana TrijayantiNo ratings yet
- 9 - Respiratory FailureDocument7 pages9 - Respiratory Failureعبدالحكيم حثولNo ratings yet
- Blood Gas AnalysisDocument31 pagesBlood Gas AnalysisBagas Dyakso DarmojoNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Arterial Blood Gas: Interpretation and Clinical ImplicationsDocument112 pagesArterial Blood Gas: Interpretation and Clinical ImplicationsmatrixtrinityNo ratings yet
- Rs4-Gas Exchange and TransportDocument5 pagesRs4-Gas Exchange and TransportGabriella ChafrinaNo ratings yet
- Arterial Blood GasDocument6 pagesArterial Blood GasnsfanfoinNo ratings yet
- Arterial Blood GasDocument33 pagesArterial Blood GaskartikaparamitaNo ratings yet
- Oxygen Solubility in Experimental Media: Oxygraph-2kDocument6 pagesOxygen Solubility in Experimental Media: Oxygraph-2kRamachandran VenkateshNo ratings yet
- Arterial Blood Gases, Ox..., Lawrence Martin, M.D.Document9 pagesArterial Blood Gases, Ox..., Lawrence Martin, M.D.mrezasyahliNo ratings yet
- Arterial Blood Gases: Laboratory InsightsDocument9 pagesArterial Blood Gases: Laboratory InsightsYusuf NugrohoNo ratings yet
- Respiratory Acid-Base DisordersDocument13 pagesRespiratory Acid-Base DisordersAlfredo PreciadoNo ratings yet
- Arterial Blood GasDocument255 pagesArterial Blood GasMark Joshua S CruzNo ratings yet
- Acido Base Critical CareDocument18 pagesAcido Base Critical CareJulia Uchoa UchoaNo ratings yet
- PCO2 Cartridge Test Information SheetDocument6 pagesPCO2 Cartridge Test Information SheetMa Louise PetateNo ratings yet
- Abg AnalysisDocument65 pagesAbg AnalysisSyed Farooque AliNo ratings yet
- Arterial Blood Gas AnalysisDocument28 pagesArterial Blood Gas Analysishendra_darmawan_4No ratings yet
- Blood Gas MachineDocument33 pagesBlood Gas MachinenofearnofearNo ratings yet
- D MystifiedDocument10 pagesD MystifiedWalaa YousefNo ratings yet
- Why Measure Blood Gases A Threepart Introduction For The Novice Part 3Document9 pagesWhy Measure Blood Gases A Threepart Introduction For The Novice Part 3Tibi TibiNo ratings yet
- Arterial Blood Gase1Document5 pagesArterial Blood Gase1meku mekuNo ratings yet
- Arterial Blood Gas Analysis - Hand OutsDocument3 pagesArterial Blood Gas Analysis - Hand OutsRANo ratings yet
- Blood Gas AnalysisDocument5 pagesBlood Gas Analysissraji64No ratings yet
- V/Q and Oxygen: Anuja Abayadeera Part 1B AnaesthsiologyDocument42 pagesV/Q and Oxygen: Anuja Abayadeera Part 1B Anaesthsiologyv_vijayakanth7656No ratings yet
- Arterial Blood GasesDocument10 pagesArterial Blood GasesSoumya BhattacharyaNo ratings yet
- Capnography in DogsDocument14 pagesCapnography in DogswalczakcNo ratings yet
- Oxygen Allows Less VentilationDocument1 pageOxygen Allows Less VentilationSyed Shahrul Naz SyedNo ratings yet
- Arterial Blood Gas.Document4 pagesArterial Blood Gas.Sathish KumarNo ratings yet
- ABG GeekymedicsDocument13 pagesABG Geekymedicscharlyn206No ratings yet
- Analisis Gas DarahDocument2 pagesAnalisis Gas DarahTri GunawanNo ratings yet
- Hydrogen Ion Concentration and PH: Basic ConceptsDocument16 pagesHydrogen Ion Concentration and PH: Basic Conceptsvanessa armeliaNo ratings yet
- BSAVA - Interpretation of Arterial Blood Gas - VINDocument5 pagesBSAVA - Interpretation of Arterial Blood Gas - VINvetthamilNo ratings yet
- Blood Gas and Acid Base AnalysisDocument1 pageBlood Gas and Acid Base AnalysisErdi TuwenoNo ratings yet
- Analisis Gas DarahDocument2 pagesAnalisis Gas DarahTri GunawanNo ratings yet
- Blood Gas Questions With Answers - 1998Document11 pagesBlood Gas Questions With Answers - 1998somarajakNo ratings yet
- Arterial Blood Gas Analysis: BY-Shivam Sachan (JR Ii) Moderator - Dr. R.K YADAV (M.D)Document52 pagesArterial Blood Gas Analysis: BY-Shivam Sachan (JR Ii) Moderator - Dr. R.K YADAV (M.D)imranqazi11No ratings yet
- Arterial Blood Gas InterpretationDocument65 pagesArterial Blood Gas InterpretationDaniel AryanNo ratings yet
- How To Interpret Arterial Blood Gas ResultsDocument9 pagesHow To Interpret Arterial Blood Gas ResultsteleasadgramNo ratings yet
- Abg Analysis ReviewerDocument21 pagesAbg Analysis ReviewerAyiessa_AJNo ratings yet
- ABGDocument45 pagesABGHasan SudirgoNo ratings yet
- Essential Respiratory Calculation: Lung Volumes, Dead Space, and Alveolar VentilationDocument6 pagesEssential Respiratory Calculation: Lung Volumes, Dead Space, and Alveolar VentilationHéctor GarcíaNo ratings yet
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Chapter 02Document3 pagesChapter 02Robert Kerwick100% (2)
- Chapter 01Document7 pagesChapter 01Robert Kerwick100% (5)
- EquationsDocument24 pagesEquationsRobert Kerwick100% (2)
- Chapter 01Document7 pagesChapter 01Robert Kerwick100% (5)
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Pa Essentials of Clinical Pathology 2010 PDF UnitedvrgDocument382 pagesPa Essentials of Clinical Pathology 2010 PDF UnitedvrgSafdar Ali67% (3)
- Introduction To ElectrolytesDocument13 pagesIntroduction To ElectrolytesMaam ShaNo ratings yet
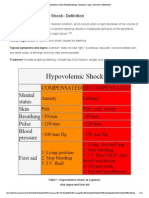
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarDocument15 pagesHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoNo ratings yet
- ABG - Simplified: Dr.S.Arun CheguevaraDocument29 pagesABG - Simplified: Dr.S.Arun CheguevaraSmilewith RakshiNo ratings yet
- Diagnosis and Management of Fetal DIstress - A Review Based On Modern Concept and Ancient Ayurvedic GranthasDocument3 pagesDiagnosis and Management of Fetal DIstress - A Review Based On Modern Concept and Ancient Ayurvedic GranthasaginaNo ratings yet
- Acid Base Balance in Critical Care Medicine-NELIGAN PDFDocument0 pagesAcid Base Balance in Critical Care Medicine-NELIGAN PDFAdistya SariNo ratings yet
- ABG ExamplesDocument31 pagesABG ExamplesKEROLOS MAHROUSNo ratings yet
- Chapter 39: Fluid, Electrolytes, and Acid-Base Balance Yoost & Crawford: Fundamentals of Nursing: Active Learning For Collaborative Practice, 2nd EditionDocument12 pagesChapter 39: Fluid, Electrolytes, and Acid-Base Balance Yoost & Crawford: Fundamentals of Nursing: Active Learning For Collaborative Practice, 2nd Editionbafraley7No ratings yet
- CCRN Synergy and Exam StartegiesDocument12 pagesCCRN Synergy and Exam StartegiesMarcus, RN100% (2)
- Arawali Veterinary College Bajor, SikarDocument8 pagesArawali Veterinary College Bajor, Sikarashish kumarNo ratings yet
- Examples of Mixed Acid-Base DisordersDocument2 pagesExamples of Mixed Acid-Base DisordersAfifa Noori SiddiquiNo ratings yet
- Acidosis and Alkalosis: Common Causes of Acid-Base DisordersDocument1 pageAcidosis and Alkalosis: Common Causes of Acid-Base DisordersErand TopalliNo ratings yet
- Case Study - NephroticDocument23 pagesCase Study - NephroticLorelyn Delfin0% (1)
- BSAVA - Interpretation of Arterial Blood Gas - VINDocument5 pagesBSAVA - Interpretation of Arterial Blood Gas - VINvetthamilNo ratings yet
- Acid Base BalanceDocument56 pagesAcid Base BalanceVirendra Joshi100% (1)
- Acid-Base Homeostasis: Clin J Am Soc Nephrol. 10.2215/CJN.07400715 26597304Document18 pagesAcid-Base Homeostasis: Clin J Am Soc Nephrol. 10.2215/CJN.07400715 26597304Christine SiraitNo ratings yet
- Acidosis and AlkalosisDocument10 pagesAcidosis and AlkalosisNealeth NanquilNo ratings yet
- UntitledDocument8 pagesUntitledYou TuberNo ratings yet
- MGR University SyllabusDocument33 pagesMGR University SyllabussanjviewsNo ratings yet
- Acute Renal Failure: John FeehallyDocument107 pagesAcute Renal Failure: John Feehallygede wira mahaditaNo ratings yet
- Nursing Practice III Care of Clients Part BDocument29 pagesNursing Practice III Care of Clients Part BAnnica Lozano100% (1)
- Inborn Errors of Metabolism in Infancy: A Guide To DiagnosisDocument11 pagesInborn Errors of Metabolism in Infancy: A Guide To DiagnosisEdu Diaperlover São PauloNo ratings yet
- Surgical ICU Exam Content OutlineDocument6 pagesSurgical ICU Exam Content OutlineDarren DawkinsNo ratings yet
- Acid Base Disorders JAPIDocument5 pagesAcid Base Disorders JAPIVitrag_Shah_1067No ratings yet
- Lab Dept: Chemistry Test Name: Lactate: General InformationDocument2 pagesLab Dept: Chemistry Test Name: Lactate: General InformationŽeljkoNo ratings yet
- IADVL Color Atlas of Dermatopathology - BookDocument41 pagesIADVL Color Atlas of Dermatopathology - Book65gkenNo ratings yet
- Causes and Evaluation of Hyperkalemia in Adults - UpToDateDocument25 pagesCauses and Evaluation of Hyperkalemia in Adults - UpToDateDaniely FreitasNo ratings yet
- The Toxicology Handbook For CliniciansDocument359 pagesThe Toxicology Handbook For Cliniciansmariposa_061280% (5)
- Lecture NotesDocument56 pagesLecture NotesLalaine April E. Ortiola100% (13)