You might also like
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki HartawanNo ratings yet
- 5 Identifying ECG IrregularitiesDocument37 pages5 Identifying ECG IrregularitiesRahmat MuliaNo ratings yet
- Copd - 2 Penting 13Document14 pagesCopd - 2 Penting 13Rahmat MuliaNo ratings yet
- 03 Pathophysiology of CommunityDocument3 pages03 Pathophysiology of CommunityVenerandaNo ratings yet
- Tinea Pedis An UpdateDocument5 pagesTinea Pedis An UpdateRahmat MuliaNo ratings yet
- J Oftalmologi Vol 7 No 1 (Heni Riyanto)Document4 pagesJ Oftalmologi Vol 7 No 1 (Heni Riyanto)Mahanani SubagioNo ratings yet
- Chapter 56Document57 pagesChapter 56Rahmat MuliaNo ratings yet
- RESPIRATORY DISORDERS (Abdurahman S)Document19 pagesRESPIRATORY DISORDERS (Abdurahman S)Rahmat MuliaNo ratings yet
- Oleh: Dr. Abdurachman Sukadi, Dr.,SpakDocument31 pagesOleh: Dr. Abdurachman Sukadi, Dr.,SpakRahmat MuliaNo ratings yet
- Tinea Pedis An UpdateDocument5 pagesTinea Pedis An UpdateRahmat MuliaNo ratings yet
- Coveram Symcard DR Yerizal PDFDocument47 pagesCoveram Symcard DR Yerizal PDFRahmat MuliaNo ratings yet
- Hidrosefalus Nonkomunikan Pada Perdarahan Intraserebral/IntraventrikularDocument2 pagesHidrosefalus Nonkomunikan Pada Perdarahan Intraserebral/IntraventrikularRahmat MuliaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
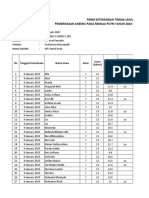
- Pemeriksaan Anemia SMP Darul MaarifDocument38 pagesPemeriksaan Anemia SMP Darul MaarifPuskesmas BanyuputihNo ratings yet
- Tropical Oceans: Word SearchDocument2 pagesTropical Oceans: Word SearchAgrobacterium TumefaciensNo ratings yet
- Pulmonary TuberculosisDocument4 pagesPulmonary TuberculosisAymen OmerNo ratings yet
- Denizdoll PatternDocument14 pagesDenizdoll PatternUmeko100% (4)
- Society of Primitive Technology - Earth Skills, Wilderness Survival (PDFDrive)Document156 pagesSociety of Primitive Technology - Earth Skills, Wilderness Survival (PDFDrive)Eng. Alexandre AlbinoNo ratings yet
- Etiology of ThrombocytosisDocument5 pagesEtiology of ThrombocytosisSimon Messi SiringoringoNo ratings yet
- SynesisDocument1 pageSynesisapi-302118481No ratings yet
- Mccracken'S Removable Partial Prosthodontics. Chapter 10 & 19Document50 pagesMccracken'S Removable Partial Prosthodontics. Chapter 10 & 19Al CarLozNo ratings yet
- IELTS Reading Lesson 4: Matching Paragraphs: Useful InformationDocument11 pagesIELTS Reading Lesson 4: Matching Paragraphs: Useful InformationTuấn Nguyễn Anh100% (1)
- Antoninus Final Exams For Lay OutDocument5 pagesAntoninus Final Exams For Lay Outmina villamor50% (2)
- DMDave - Dungeons & Lairs #30 Owlbear Wood (April 2023 Revision)Document8 pagesDMDave - Dungeons & Lairs #30 Owlbear Wood (April 2023 Revision)Rodrigo X. FiorinNo ratings yet
- Case PresentationDocument11 pagesCase PresentationJOhn DiCeNo ratings yet
- Feed Refernce Standard in The PhilippinesDocument3 pagesFeed Refernce Standard in The PhilippinesbbandojaNo ratings yet
- The Mice That Set The Elephants FreeDocument2 pagesThe Mice That Set The Elephants FreePeter LuaNo ratings yet
- Dark Hunters PDFDocument5 pagesDark Hunters PDFMatthew HaydenNo ratings yet
- FeygodsDocument6 pagesFeygodsZhori DuberryNo ratings yet
- Cloze Test VocabDocument15 pagesCloze Test VocabSurachai Rodngam100% (1)
- 1 SMDocument10 pages1 SMNurul Hikmah Haetapi AminNo ratings yet
- A Hebrew Primer BallDocument288 pagesA Hebrew Primer Ballondoveo4749No ratings yet
- Diabetes Mellitus (DM) 2Document1 pageDiabetes Mellitus (DM) 2Bheru Lal100% (1)
- Output RAISEPlanDocument4 pagesOutput RAISEPlanLovely Venia JovenNo ratings yet
- Musical Instruments of AfricaDocument3 pagesMusical Instruments of AfricaSitti Nur HabingNo ratings yet
- Artículo de Royal Canin - The Barf Trend Advantages, Drawbacks and RisksDocument8 pagesArtículo de Royal Canin - The Barf Trend Advantages, Drawbacks and RisksAlejandra CárdenasNo ratings yet
- PPG Reviewer For ShsDocument5 pagesPPG Reviewer For ShsGoldwin RamirezNo ratings yet
- 1cambridge English Prepare 3 WorkbookDocument90 pages1cambridge English Prepare 3 WorkbookMariana Villalón100% (1)
- Under The Sparkling SeaDocument48 pagesUnder The Sparkling SeaCreepygamer this is power100% (3)
- Laser Enhancement ProtocolsDocument25 pagesLaser Enhancement ProtocolsWolfManNo ratings yet
- 100 Years of ZsiDocument5 pages100 Years of ZsiAshutoshkumar jhaNo ratings yet
- 4TH Periodical Test in English 2018-2019Document6 pages4TH Periodical Test in English 2018-2019Jhun Tandang100% (1)
- 2001 LamenessDocument112 pages2001 LamenessZozo Mostafa100% (1)