You might also like
- Discharge Summary TemplateDocument1 pageDischarge Summary TemplateRinson JosephNo ratings yet
- Diagnosis: Acute GastroenteritisDocument1 pageDiagnosis: Acute GastroenteritisSakshi RanabhatNo ratings yet
- Hospital Discharge SummaryDocument1 pageHospital Discharge SummaryprofarmahNo ratings yet
- Medical Billing SlidesDocument16 pagesMedical Billing SlidesSam matthieuNo ratings yet
- Cholecystitis - Discharge SummaryDocument1 pageCholecystitis - Discharge SummaryIndranil SinhaNo ratings yet
- Discharge-Summary-Template JogiDocument1 pageDischarge-Summary-Template JogiJoginderNo ratings yet
- Gynae Care Plan ECTOPIC ReviewedDocument2 pagesGynae Care Plan ECTOPIC ReviewedDet LaurenteNo ratings yet
- Fifty Questions For Family History InterviewsDocument4 pagesFifty Questions For Family History InterviewsRodrigo Muñoz JimenezNo ratings yet
- Self Pay Information FormDocument1 pageSelf Pay Information FormPerformax Physical TherapyNo ratings yet
- How Become A SurgeonDocument15 pagesHow Become A SurgeonBárbara LeiteNo ratings yet
- Surgery Short QuestionsDocument22 pagesSurgery Short QuestionsDevanshNo ratings yet
- Memorial Hermann Discharge Papers - 3Document5 pagesMemorial Hermann Discharge Papers - 3Alaska JamesNo ratings yet
- Doctor Job Description Position Title DoctorDocument4 pagesDoctor Job Description Position Title DoctorBianca Andreea BalintNo ratings yet
- Scope of Nursing PracticeDocument30 pagesScope of Nursing PracticeVandyck Agyemang JuniorNo ratings yet
- What Doctors Myy Not Tell You About Psychiatric DrugsDocument18 pagesWhat Doctors Myy Not Tell You About Psychiatric DrugsDhwani ShahNo ratings yet
- Acute PericarditisDocument8 pagesAcute Pericarditisalina abu rumiNo ratings yet
- Nursing Student Handbook 2020-2021Document41 pagesNursing Student Handbook 2020-2021serbo81No ratings yet
- Medication Plan and Discharge SummaryDocument9 pagesMedication Plan and Discharge SummaryZaharia AlexandrNo ratings yet
- Emergency Room Assessment Form: Best Eye Opening Best VerbalDocument2 pagesEmergency Room Assessment Form: Best Eye Opening Best Verbaleliza marie luisNo ratings yet
- Corneal DystrophyDocument5 pagesCorneal DystrophyDejan JanevNo ratings yet
- Phi RythmDocument6 pagesPhi RythmStanley IgweNo ratings yet
- Resume of SwahrerDocument2 pagesResume of Swahrerapi-23955632No ratings yet
- Guide For Refund of Bid SecurityDocument2 pagesGuide For Refund of Bid SecurityPragya281850% (2)
- Midwifery - SterlizationDocument39 pagesMidwifery - SterlizationEsha KuttiNo ratings yet
- Tubal LigationDocument3 pagesTubal LigationPal_inNo ratings yet
- Sterilization Fertilization Isth Mic Portion of The Fallopian TubeDocument3 pagesSterilization Fertilization Isth Mic Portion of The Fallopian TubeRj FloresNo ratings yet
- Advanced Laparoscopic Hysterectomy SurgeryDocument2 pagesAdvanced Laparoscopic Hysterectomy SurgeryManu GynecologyNo ratings yet
- Tubal LigationDocument3 pagesTubal LigationVOn Calda VidalNo ratings yet
- Surgical Management For Endrometriotic CystsDocument4 pagesSurgical Management For Endrometriotic CystsLadybelle GototosNo ratings yet
- TAH and BSO (TAH-BSO) Is Still Considered The Standard Operative Procedure For Patients With Endometrial CancerDocument3 pagesTAH and BSO (TAH-BSO) Is Still Considered The Standard Operative Procedure For Patients With Endometrial CancerVanessa VillanuevaNo ratings yet
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop: Why Do I Need This Surgery?Document6 pagesUrinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop: Why Do I Need This Surgery?Panji SetyawanNo ratings yet
- Cs With BTLDocument16 pagesCs With BTLSteffiNo ratings yet
- VasectomyDocument20 pagesVasectomyAngelica MaeNo ratings yet
- SuegeryDocument3 pagesSuegeryCristian VieriuNo ratings yet
- Type of SurgeryDocument5 pagesType of SurgeryNormala Macabuntal SaripadaNo ratings yet
- Hysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Common Surgical Procedures AssignmentDocument3 pagesCommon Surgical Procedures AssignmentDreamy AspirationsNo ratings yet
- CancerDocument10 pagesCancercitidotnetNo ratings yet
- Gynecological Surgery - Sundhed - DKDocument19 pagesGynecological Surgery - Sundhed - DKPavel BerlinschiNo ratings yet
- CystectomyDocument3 pagesCystectomyJorie Muedan RamirezNo ratings yet
- Mastectomy Case StudyDocument9 pagesMastectomy Case StudyAura Regene AtienzaNo ratings yet
- Tubal SterilizationDocument104 pagesTubal Sterilization3rd yrsNo ratings yet
- Total Abdominal Hysterectomy Bilateral SaphingoDocument7 pagesTotal Abdominal Hysterectomy Bilateral SaphingoAndrea BroccoliNo ratings yet
- What Is Bilateral Tubal LigationDocument42 pagesWhat Is Bilateral Tubal LigationAldrich ArquizaNo ratings yet
- Surgical WardDocument28 pagesSurgical Wardyamie sulongNo ratings yet
- TAHBSODocument3 pagesTAHBSOakatzkiNo ratings yet
- HysterectomyDocument5 pagesHysterectomysapana shah100% (1)
- Cholecystectomy (: Laparoscopic GallstonesDocument4 pagesCholecystectomy (: Laparoscopic GallstonesAlexia BatungbacalNo ratings yet
- SurgeryDocument1 pageSurgeryJoannalyn Libo-onNo ratings yet
- Laparoscopy: Women's Health Information For PatientsDocument8 pagesLaparoscopy: Women's Health Information For PatientsKamran AfzalNo ratings yet
- BTL ReportDocument9 pagesBTL ReportmhelcizNo ratings yet
- Consent For Laparoscopic Hysterectomy EnglishDocument4 pagesConsent For Laparoscopic Hysterectomy EnglishGaurav AroraNo ratings yet
- Exploratory LaparotomyDocument25 pagesExploratory Laparotomywinai13No ratings yet
- SCP BSUG July 2017Document15 pagesSCP BSUG July 2017Yasir K. HaniNo ratings yet
- HysterectomyDocument3 pagesHysterectomyRobesito Evangelista ArtiagaNo ratings yet
- Specialist Gynaecologist Hamilton Waikato NZ 3204Document3 pagesSpecialist Gynaecologist Hamilton Waikato NZ 3204joe richardNo ratings yet
- Clinical Case Analysis Ectopic PregnancyDocument4 pagesClinical Case Analysis Ectopic PregnancySiobhan GreeneNo ratings yet
- Hysteroscopic Surgeries: What Is Hysteroscopic Medical Procedure?Document4 pagesHysteroscopic Surgeries: What Is Hysteroscopic Medical Procedure?AltiusHospitalNo ratings yet
- Summary Evaluation of Laboratory WorksDocument2 pagesSummary Evaluation of Laboratory WorksBerna PielagoNo ratings yet
- Health Perception and Management PatternDocument3 pagesHealth Perception and Management PatternBerna PielagoNo ratings yet
- T5R1Document1 pageT5R1Berna PielagoNo ratings yet
- Health Perception and Management PatternDocument3 pagesHealth Perception and Management PatternBerna PielagoNo ratings yet
- PE (Basic Steps)Document6 pagesPE (Basic Steps)Berna Pielago100% (7)
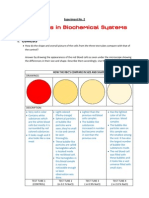
- Experiment No. 2Document5 pagesExperiment No. 2Berna Pielago67% (6)
- Towards A Sociology of Health Discourse in AfricaDocument172 pagesTowards A Sociology of Health Discourse in AfricaDavid Polowiski100% (2)
- The Only Book A Teen Will EVER Need To Lose Fat & Build Muscle in The GymDocument146 pagesThe Only Book A Teen Will EVER Need To Lose Fat & Build Muscle in The GymJake Farrugia100% (1)
- Dr. Sudarto Sppd's FileDocument22 pagesDr. Sudarto Sppd's FileVindy CesarianaNo ratings yet
- SNB Exam Sample Question Paper 2Document19 pagesSNB Exam Sample Question Paper 2Ketheesaran LingamNo ratings yet
- Aldrine Ilustricimo VS Nyk Fil Sjip Management IncDocument11 pagesAldrine Ilustricimo VS Nyk Fil Sjip Management Inckristel jane caldozaNo ratings yet
- Deadly Deception - Robert WillnerDocument303 pagesDeadly Deception - Robert Willnerleocarvalho001_60197100% (5)
- Illness in The NewbornDocument34 pagesIllness in The NewbornVivian Jean TapayaNo ratings yet
- Aerodrome Emergency Plan PresentationDocument22 pagesAerodrome Emergency Plan PresentationalexlytrNo ratings yet
- Is It True That GanodermaDocument2 pagesIs It True That GanodermaRohit SharmaNo ratings yet
- Cholecystitis BelgradeDocument52 pagesCholecystitis BelgradeLazar VučetićNo ratings yet
- Subjective: Diarrhea Related To Watery Short Term: IndependentDocument4 pagesSubjective: Diarrhea Related To Watery Short Term: IndependentEmma Lyn SantosNo ratings yet
- Cardiology - Corrected AhmedDocument23 pagesCardiology - Corrected AhmedHanadi UmhanayNo ratings yet
- Meralgia ParaestheticaDocument4 pagesMeralgia ParaestheticaNatalia AndronicNo ratings yet
- Principles - of - Genetics 6th Ed by Snustad - 20 (PDF - Io) (PDF - Io) - 12-14-1-2Document2 pagesPrinciples - of - Genetics 6th Ed by Snustad - 20 (PDF - Io) (PDF - Io) - 12-14-1-2Ayu JumainNo ratings yet
- The Analysis and Reflection On That Sugar FilmDocument2 pagesThe Analysis and Reflection On That Sugar FilmkkkkNo ratings yet
- Paper Roleplay Group 3Document7 pagesPaper Roleplay Group 3Endah Ragil SaputriNo ratings yet
- QB BT PDFDocument505 pagesQB BT PDFنيزو اسوNo ratings yet
- Abnormal Psychology Final Practice QuestionsDocument16 pagesAbnormal Psychology Final Practice QuestionsJames WilkesNo ratings yet
- DSM OcdDocument2 pagesDSM Ocdnmyza89No ratings yet
- Arthur CrawfordDocument308 pagesArthur CrawfordRupali Mokashi100% (1)
- Annex I Summary of Product CharacteristicsDocument29 pagesAnnex I Summary of Product CharacteristicslisnerisNo ratings yet
- China Animal Healthcare: The Healing TouchDocument19 pagesChina Animal Healthcare: The Healing TouchBin WeiNo ratings yet
- USA V Ronald Phillip Wallace Case 1:08-cr-00409-CMA Document 85 Filed 05/14/12 USDC ColoradoDocument71 pagesUSA V Ronald Phillip Wallace Case 1:08-cr-00409-CMA Document 85 Filed 05/14/12 USDC ColoradoRob SNo ratings yet
- Blood Can Be Very BadDocument37 pagesBlood Can Be Very BadPhil SingerNo ratings yet
- Week 1 - NCMA 219 LecDocument27 pagesWeek 1 - NCMA 219 LecDAVE BARIBENo ratings yet
- Factsheet - Ectopic Heartbeats (160201)Document1 pageFactsheet - Ectopic Heartbeats (160201)RodiAdiNo ratings yet
- Research ProposalDocument45 pagesResearch ProposalBoruuf If GammachuuNo ratings yet
- HEX PG SyllabusDocument124 pagesHEX PG SyllabusJegadeesan MuniandiNo ratings yet
- 11 Retention of Maxillofacial Prosthesis Fayad PDFDocument7 pages11 Retention of Maxillofacial Prosthesis Fayad PDFMostafa Fayad50% (2)
- Bipolar Disorder - A Cognitive Therapy Appr - Cory F. NewmanDocument283 pagesBipolar Disorder - A Cognitive Therapy Appr - Cory F. NewmanAlex P100% (1)