You might also like
- LVL 1 The Slaying StoneDocument34 pagesLVL 1 The Slaying StoneArturo Partida95% (19)
- Assignment of Constitutional Law Topic-State Under Article 12Document21 pagesAssignment of Constitutional Law Topic-State Under Article 12Saba AfreenNo ratings yet
- The Metabolic SyndromeDocument37 pagesThe Metabolic SyndromeRoby Kieran100% (1)
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseFrom EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNo ratings yet
- Disorders of Lipid Metabolism LectureDocument55 pagesDisorders of Lipid Metabolism LectureRichard SiahaanNo ratings yet
- Jurnal HyperlipidemiaDocument12 pagesJurnal HyperlipidemiaJo LenongNo ratings yet
- DZIELSKA MARIA 1996 Hypatia of Alexandria (Harvard University Press)Document180 pagesDZIELSKA MARIA 1996 Hypatia of Alexandria (Harvard University Press)ivory2011100% (3)
- DEED OF SALE OF MOTOR VEHICLE - TemplateDocument1 pageDEED OF SALE OF MOTOR VEHICLE - TemplateLiz BorromeoNo ratings yet
- Manantan v. CADocument1 pageManantan v. CARywNo ratings yet
- Soulmate SecretDocument5 pagesSoulmate SecretOla OlaNo ratings yet
- HELLP SYNDROME: A LIFE-THREATENING PREGNANCY COMPLICATIONDocument10 pagesHELLP SYNDROME: A LIFE-THREATENING PREGNANCY COMPLICATIONFenshiro LesnussaNo ratings yet
- Fast Facts: Hyperlipidemia: Bringing clarity to lipid managementFrom EverandFast Facts: Hyperlipidemia: Bringing clarity to lipid managementNo ratings yet
- Clinical Pathology NotesDocument82 pagesClinical Pathology NotesCésar HelenoNo ratings yet
- Smu02b v300r002c02 User Manual 02Document248 pagesSmu02b v300r002c02 User Manual 02Jaime Andres Niño100% (2)
- Part and Mold Design GuideDocument170 pagesPart and Mold Design GuideminhtintinNo ratings yet
- Admin Case DigestDocument8 pagesAdmin Case DigestlenvfNo ratings yet
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitNo ratings yet
- Lipid Metabolism - 3rd LectureDocument38 pagesLipid Metabolism - 3rd LectureLe Uyen Nguyen100% (1)
- R69 Sepulveda V PelaezDocument2 pagesR69 Sepulveda V PelaezfranceheartNo ratings yet
- Dyslipidemia PDFDocument28 pagesDyslipidemia PDFwilliaNo ratings yet
- Connectors of Addition and ContrastDocument2 pagesConnectors of Addition and Contrastmmaarr100% (2)
- HypertriglyceridemiaDocument8 pagesHypertriglyceridemiaNaila KhanNo ratings yet
- 0043 PDFDocument17 pages0043 PDFZuhdan AnnajmutstsaqibNo ratings yet
- CVS HYPERLIPIDEMIASNew Microsoft Office PowerPoint PresentationDocument19 pagesCVS HYPERLIPIDEMIASNew Microsoft Office PowerPoint Presentationmizramaqsood347No ratings yet
- 3 s2.0 B9780128158449000087 MainDocument33 pages3 s2.0 B9780128158449000087 MainBlanca LozanoNo ratings yet
- LipoproteinemiaDocument50 pagesLipoproteinemiaShajeer Salim67% (6)
- A Neonatal Hypertriglyceridemia Presenting With ReDocument3 pagesA Neonatal Hypertriglyceridemia Presenting With ReIndahNo ratings yet
- Nutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94Document13 pagesNutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94mmmdeandradeNo ratings yet
- Lipid Profile: Dr. MD Razib HasanDocument26 pagesLipid Profile: Dr. MD Razib HasanRazib HasanNo ratings yet
- Lipodistrofia FamiliarDocument4 pagesLipodistrofia FamiliarKaren Magalí CruzNo ratings yet
- Dislipidemia Lancet Durrington PDFDocument15 pagesDislipidemia Lancet Durrington PDFAlphaJulissa JuarezNo ratings yet
- Lipids in Health and DiseaseDocument5 pagesLipids in Health and DiseaseDwika DhiandriNo ratings yet
- DyslipidaemiaDocument34 pagesDyslipidaemiaMusfique RashidNo ratings yet
- Assessment of jaundice causes and evaluationDocument16 pagesAssessment of jaundice causes and evaluationlaura canoNo ratings yet
- Colangitis FelinaDocument22 pagesColangitis FelinaJuan K SeguraNo ratings yet
- J CLD 2017 08 007Document15 pagesJ CLD 2017 08 007Nicolas AdrianoNo ratings yet
- 0043 PDFDocument12 pages0043 PDFZuhdan AnnajmutstsaqibNo ratings yet
- Dyslipidemia: LipoproteinDocument25 pagesDyslipidemia: LipoproteinNarayananNo ratings yet
- Understanding Lipoprotein MetabolismDocument10 pagesUnderstanding Lipoprotein MetabolismroropujiNo ratings yet
- Armstrong 2009Document18 pagesArmstrong 2009Guilherme de FreitasNo ratings yet
- Metabolic Syndrome - Overview and Current GuidelinesDocument12 pagesMetabolic Syndrome - Overview and Current GuidelinessserggiosNo ratings yet
- Fisiopatologia Sindrome MetabolicoDocument9 pagesFisiopatologia Sindrome MetabolicoEmilio MoncadaNo ratings yet
- Notes Chapter 35Document16 pagesNotes Chapter 35Christene GVNo ratings yet
- Lipid and LipoproteinsDocument4 pagesLipid and LipoproteinsDIEGO RAFAEL ESPIRITUNo ratings yet
- DD Metabolic SyndromeDocument5 pagesDD Metabolic SyndromeEluNo ratings yet
- Hypertriglyceridemia: Practice Essentials, Pathophysiology, EtiologyDocument18 pagesHypertriglyceridemia: Practice Essentials, Pathophysiology, EtiologyDr Praveen PrashantNo ratings yet
- Jaundiceandpregnancy JIACMDocument7 pagesJaundiceandpregnancy JIACMHaekal HafizhNo ratings yet
- Pseudohyponatremia Nejm CpsDocument7 pagesPseudohyponatremia Nejm CpshoneyworksNo ratings yet
- Lipoprotein Metabolism: Chylomicrons, VLDL, LDL, HDLDocument32 pagesLipoprotein Metabolism: Chylomicrons, VLDL, LDL, HDLMilkoo sabaNo ratings yet
- EndocrineDocument203 pagesEndocrineSeli WondaleNo ratings yet
- Hypolipidemic Drugs 150723Document149 pagesHypolipidemic Drugs 150723istiak.imon1511722612No ratings yet
- Obesida ArticuloDocument5 pagesObesida ArticuloZangre AzulNo ratings yet
- Hyperlipidemia DR Onwe 2015Document9 pagesHyperlipidemia DR Onwe 2015ImelNo ratings yet
- Diabetes and Pancreatic TumorsDocument20 pagesDiabetes and Pancreatic TumorsleahbayNo ratings yet
- 22 - Hypolipdemic DrugsDocument64 pages22 - Hypolipdemic Drugsmashe1No ratings yet
- Vetcpd Adrenal Disease Notes Christopher Scudder BVSC (Dist) Mvetmed (Dist) PHD Dipacvim Mrcvs Christopher - Scudder@Southfields - Co.UkDocument21 pagesVetcpd Adrenal Disease Notes Christopher Scudder BVSC (Dist) Mvetmed (Dist) PHD Dipacvim Mrcvs Christopher - Scudder@Southfields - Co.UkStefana UrsuNo ratings yet
- Chapter 24 - DylipidaemiaDocument7 pagesChapter 24 - DylipidaemiaMark Harold GonzalesNo ratings yet
- NAFLDDocument41 pagesNAFLDSakshiNo ratings yet
- Elevated Lactic Acid During Ketoacidosis: Pathophysiology and ManagementDocument3 pagesElevated Lactic Acid During Ketoacidosis: Pathophysiology and ManagementMega RangganizerNo ratings yet
- Cholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfDocument30 pagesCholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfNeha MasarkarNo ratings yet
- LipidDocument31 pagesLipidahmed abd elazizNo ratings yet
- Metabolic SyndromeDocument55 pagesMetabolic SyndromeAakash BalasubramanianNo ratings yet
- Clinical diagnosis of dyslipidaemia and familial hypercholesterolaemiaDocument9 pagesClinical diagnosis of dyslipidaemia and familial hypercholesterolaemiaangelmedurNo ratings yet
- PHS 309-Pancreatic Hormones-1Document36 pagesPHS 309-Pancreatic Hormones-1kinghenry882No ratings yet
- Pathogenesis of NAFLD ExplainedDocument48 pagesPathogenesis of NAFLD Explainedsudipta kumarNo ratings yet
- HyperlipidemiaDrOnwe2015 PDFDocument9 pagesHyperlipidemiaDrOnwe2015 PDFZainab AliNo ratings yet
- The Hellp Syndrome - A Therapeutic ChallengeDocument41 pagesThe Hellp Syndrome - A Therapeutic Challengeد. أحمد عبد الباسطNo ratings yet
- Test 1 - Psio303aDocument28 pagesTest 1 - Psio303aErika Aranda0% (1)
- YounisDocument12 pagesYounisSaadNo ratings yet
- Clinical SignificanceDocument31 pagesClinical Significancejav israelNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
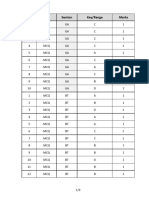
- Q.No. Type Section Key/Range MarksDocument3 pagesQ.No. Type Section Key/Range Marksbiotech_vidhyaNo ratings yet
- Stripping For ReprobingDocument2 pagesStripping For ReprobingStella SalvatoreNo ratings yet
- Brad FordDocument12 pagesBrad FordQi ChaoNo ratings yet
- Facs ProtocolDocument7 pagesFacs ProtocolmisterxNo ratings yet
- BT 2019Document13 pagesBT 2019biotech_vidhyaNo ratings yet
- Stripping For ReprobingDocument2 pagesStripping For ReprobingStella SalvatoreNo ratings yet
- Troubleshooting SDS-PAGE 1Document3 pagesTroubleshooting SDS-PAGE 1biotech_vidhyaNo ratings yet
- Polymerasen GuideDocument16 pagesPolymerasen Guidebiotech_vidhyaNo ratings yet
- Nuclear ExtractsDocument2 pagesNuclear Extractsbiotech_vidhyaNo ratings yet
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocument6 pagesBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaNo ratings yet
- Whole Cell ExtractDocument1 pageWhole Cell Extractbiotech_vidhyaNo ratings yet
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocument6 pagesBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaNo ratings yet
- SDS PageDocument2 pagesSDS Pagebiotech_vidhyaNo ratings yet
- Components Reaction MixtureDocument3 pagesComponents Reaction Mixturebiotech_vidhyaNo ratings yet
- Ies 17 Set A Me Q ADocument67 pagesIes 17 Set A Me Q Abiotech_vidhyaNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- Polymerase Chain Reaction (PCR)Document3 pagesPolymerase Chain Reaction (PCR)biotech_vidhyaNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- Qpaper PondyDocument21 pagesQpaper Pondybiotech_vidhyaNo ratings yet
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaNo ratings yet
- ESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionDocument52 pagesESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionpataNo ratings yet
- TDC 41597 A (Mechanical Engg.) - 2012Document20 pagesTDC 41597 A (Mechanical Engg.) - 2012biotech_vidhyaNo ratings yet
- Mechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010Document20 pagesMechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010biotech_vidhyaNo ratings yet
- Befcv List PDFDocument22 pagesBefcv List PDFbiotech_vidhyaNo ratings yet
- Qpaper PondyDocument21 pagesQpaper Pondybiotech_vidhyaNo ratings yet
- A.E. (Mechanical Engineering I) 2007Document24 pagesA.E. (Mechanical Engineering I) 2007Mukesh KumarNo ratings yet
- Img Word-To PDFDocument3 pagesImg Word-To PDFbiotech_vidhyaNo ratings yet
- Recruitment RulesDocument5 pagesRecruitment Rulesbiotech_vidhyaNo ratings yet
- 1 TolerancesDocument1 page1 Tolerancesbiotech_vidhyaNo ratings yet
- Graduation Day 2018 ScriptDocument3 pagesGraduation Day 2018 ScriptRiolyn Jhane Kho Ardena100% (1)
- N039-N040 Rejano Nursing Care PlanDocument3 pagesN039-N040 Rejano Nursing Care PlanBianca Marithè RejanoNo ratings yet
- Sourcing Rules in PurchasingDocument21 pagesSourcing Rules in Purchasingpradhan.neeladriNo ratings yet
- Talent ManagementDocument8 pagesTalent Managementyared haftuNo ratings yet
- Case StudyDocument14 pagesCase StudyAdel AbdulrhmanNo ratings yet
- ChatGpt For AccountantsDocument29 pagesChatGpt For Accountantssamreen khanNo ratings yet
- Gle RubricDocument1 pageGle Rubricapi-207519916No ratings yet
- Literary Terms: Literatura/litteratura (Derived Itself From Littera: Letter or Handwriting)Document2 pagesLiterary Terms: Literatura/litteratura (Derived Itself From Littera: Letter or Handwriting)Berr WalidNo ratings yet
- Module 1 MC4 LOGIC CRITICAL THINKINGDocument6 pagesModule 1 MC4 LOGIC CRITICAL THINKINGAubrey Ante100% (1)
- Stafford Beer - The World We ManageDocument12 pagesStafford Beer - The World We ManageRaoul LundbergNo ratings yet
- Gomez FL Bar Complaint v. PerezDocument6 pagesGomez FL Bar Complaint v. PerezJudgeHSNo ratings yet
- APMP SyllabusDocument20 pagesAPMP SyllabuscapsfastNo ratings yet
- Đề Thi và Đáp ÁnDocument19 pagesĐề Thi và Đáp ÁnTruong Quoc TaiNo ratings yet
- 028 - Chapter 6 - L20 PDFDocument11 pages028 - Chapter 6 - L20 PDFRevathiNo ratings yet
- Marina OneshotDocument11 pagesMarina OneshotchewyeblossomNo ratings yet
- Curriculum Vitae: Radhey ShyamDocument3 pagesCurriculum Vitae: Radhey ShyamGaurav SinghNo ratings yet
- Steps in Formatting Windows 7Document2 pagesSteps in Formatting Windows 7Marc RiomalosNo ratings yet
- ECKHOFF, Hanne & Dag Haug - Aspect and Prefixation in Old Church Slavonic PDFDocument45 pagesECKHOFF, Hanne & Dag Haug - Aspect and Prefixation in Old Church Slavonic PDFaurimiaNo ratings yet
- 07Document30 pages07David MontoyaNo ratings yet
- Plotting and Model Building in MATLABDocument30 pagesPlotting and Model Building in MATLABMuhammad Shehzad KamalNo ratings yet