You might also like
- Congenital Adrenal HyperplasiaDocument13 pagesCongenital Adrenal Hyperplasiaashgee1No ratings yet
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementFrom EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNo ratings yet
- Epidemiology and Initial Management of Ambiguous Genitalia at Birth in GermanyDocument9 pagesEpidemiology and Initial Management of Ambiguous Genitalia at Birth in GermanyFikri Abd AzisNo ratings yet
- Intersex or Disorders of Sexual DevelopmentDocument19 pagesIntersex or Disorders of Sexual DevelopmentHUSAMNo ratings yet
- Pre 2Document3 pagesPre 2hhzeipysnmgmreisioNo ratings yet
- Screening for congenital adrenal hyperplasia: low PPV and variable incidenceDocument32 pagesScreening for congenital adrenal hyperplasia: low PPV and variable incidencesalihaNo ratings yet
- Genetic counseling for polycystic kidney diseaseDocument4 pagesGenetic counseling for polycystic kidney diseaseviorel003No ratings yet
- Insight Into The Pathogensis of Polycystic OvarianDocument10 pagesInsight Into The Pathogensis of Polycystic OvarianHAVIZ YUADNo ratings yet
- Factor V Leiden and pre-eclampsia riskDocument8 pagesFactor V Leiden and pre-eclampsia riskNur Ainatun NadrahNo ratings yet
- Polycysticovarysyndrome Inadolescents: Selma Feldman Witchel,, Hailey Roumimper,, Sharon OberfieldDocument16 pagesPolycysticovarysyndrome Inadolescents: Selma Feldman Witchel,, Hailey Roumimper,, Sharon OberfieldAgustina S. SelaNo ratings yet
- Prognostic Factors and Clinical Features in Liveborn Neonates With Hydrops FetalisDocument6 pagesPrognostic Factors and Clinical Features in Liveborn Neonates With Hydrops FetalisWulan CerankNo ratings yet
- Case Report CAHDocument9 pagesCase Report CAHkhairunnisa roliNo ratings yet
- 2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno TeratozoospermiaDocument12 pages2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno Teratozoospermiakong_666064846No ratings yet
- Clinical, Biological and Genetic Analysis of Anorchia in 26 BoysDocument5 pagesClinical, Biological and Genetic Analysis of Anorchia in 26 Boysarda_ccerNo ratings yet
- A CLINICAL CASE OF A PRIMARY PARTIAL EMPTY SELLA PRESENTING WITH HYPOGONADOTROPIC HYPOGONADISMDocument4 pagesA CLINICAL CASE OF A PRIMARY PARTIAL EMPTY SELLA PRESENTING WITH HYPOGONADOTROPIC HYPOGONADISMIJAR JOURNALNo ratings yet
- Laboratory and Radiographic Tests For Ambiguous GenitaliaDocument8 pagesLaboratory and Radiographic Tests For Ambiguous GenitaliaMaria Lucia RossiNo ratings yet
- Hiperplasis Congenita AFRICADocument6 pagesHiperplasis Congenita AFRICAnadiaNo ratings yet
- Pure Gonadal Dysgenesis: Clinical Case and Review of The LiteratureDocument4 pagesPure Gonadal Dysgenesis: Clinical Case and Review of The LiteratureIJAR JOURNALNo ratings yet
- Hughes2012 PDFDocument5 pagesHughes2012 PDFJulianaNo ratings yet
- Ambiguous Genitalia Diagnosis and ManagementDocument8 pagesAmbiguous Genitalia Diagnosis and ManagementnasibdinNo ratings yet
- Maple Syrup Urine Disease Case StudyDocument5 pagesMaple Syrup Urine Disease Case StudyMaria ClaraNo ratings yet
- Nej Mo A 0911064Document11 pagesNej Mo A 0911064Marzuqi AbdullahNo ratings yet
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDocument10 pagesKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNo ratings yet
- Diagnóstico Del SopDocument13 pagesDiagnóstico Del SopxcarlosfxNo ratings yet
- Chang 2020Document13 pagesChang 2020Fernando Silva RivasNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Prenatal Diagnosis of Sex Differentiation DisorderDocument8 pagesPrenatal Diagnosis of Sex Differentiation DisorderHorvath AlexandraNo ratings yet
- Universal Screening For Familial Hypercholesterolemia I 2022 Genetics in MedDocument9 pagesUniversal Screening For Familial Hypercholesterolemia I 2022 Genetics in Medronaldquezada038No ratings yet
- Neuroendocrine Disorders in ChildrenFrom EverandNeuroendocrine Disorders in ChildrenMehul DattaniNo ratings yet
- Dor 2Document10 pagesDor 2Alce Alce EverdienNo ratings yet
- Hypertrophy of The Clitoris in An Adult Woman (Case Report)Document4 pagesHypertrophy of The Clitoris in An Adult Woman (Case Report)IJAR JOURNALNo ratings yet
- Female Genomics Infertility and Overall Health Joshi 2017Document8 pagesFemale Genomics Infertility and Overall Health Joshi 2017Orlando CuellarNo ratings yet
- MTHFR Genetic Polymorphism and The Risk of Intrauterine Fetal Death in Polish WomenDocument6 pagesMTHFR Genetic Polymorphism and The Risk of Intrauterine Fetal Death in Polish WomenMauro Porcel de PeraltaNo ratings yet
- Emergency Medicine Myths: Ectopic Pregnancy Evaluation, Risk Factors, and PresentationDocument10 pagesEmergency Medicine Myths: Ectopic Pregnancy Evaluation, Risk Factors, and PresentationJanetta RheaNo ratings yet
- Andersen Et Al 2019Document14 pagesAndersen Et Al 2019Emil AndersenNo ratings yet
- Prenatal diagnosis of genetic diseasesDocument11 pagesPrenatal diagnosis of genetic diseasesMini PGNo ratings yet
- 6 PGS缩短受孕时间Document8 pages6 PGS缩短受孕时间zjuwindNo ratings yet
- How Far Should We Explore Hypospadias? Next-Generation Sequencing Applied To A Large Cohort of Hypospadiac PatientsDocument9 pagesHow Far Should We Explore Hypospadias? Next-Generation Sequencing Applied To A Large Cohort of Hypospadiac Patientsddd gdhNo ratings yet
- 03TES2011Document999 pages03TES2011Ahmad IsmatullahNo ratings yet
- Fertility issues in disorders of sex developmentDocument15 pagesFertility issues in disorders of sex developmentEletícia SousaNo ratings yet
- Pre EklampsiaDocument21 pagesPre EklampsiaRocky.84No ratings yet
- Journal Noonan SyndromeDocument7 pagesJournal Noonan SyndromeSheilla GiustiNo ratings yet
- Crypt Orchid Is M 2014Document6 pagesCrypt Orchid Is M 2014rohitNo ratings yet
- The Human Tubal Lavage Proteome Reveals Biological Processes That May Govern The Pathology of HydrosalpinxDocument13 pagesThe Human Tubal Lavage Proteome Reveals Biological Processes That May Govern The Pathology of Hydrosalpinxrika syofianNo ratings yet
- Congenital Anomalies in Infant With Congenital HypothyroidismDocument4 pagesCongenital Anomalies in Infant With Congenital HypothyroidismAtika SugiartoNo ratings yet
- Pharmacologic Management of AntiMDA5 Quickly Progressive Interstitial Bronchi Diseasesfnwr PDFDocument1 pagePharmacologic Management of AntiMDA5 Quickly Progressive Interstitial Bronchi Diseasesfnwr PDFheliumcast26No ratings yet
- Conjugated Hyperbilirubinemia in The Neonatal Intensive Care UnitDocument9 pagesConjugated Hyperbilirubinemia in The Neonatal Intensive Care UnitIvan HoNo ratings yet
- Dermatologia: Anais Brasileiros deDocument7 pagesDermatologia: Anais Brasileiros deamanda conorattoNo ratings yet
- Microalbuminuria Predicts Mortality in ElderlyDocument4 pagesMicroalbuminuria Predicts Mortality in Elderlyilma_ilemNo ratings yet
- Prenatal Imaging Features Suggestive of Liver Gestational Allo Immune DiseaseDocument4 pagesPrenatal Imaging Features Suggestive of Liver Gestational Allo Immune DiseaseEuis NoorhayatyNo ratings yet
- v13 p74 EthicalDocument7 pagesv13 p74 EthicalVincent FloraNo ratings yet
- Prenatal Genetic Screening DBiagnosis Hamamy 2010Document27 pagesPrenatal Genetic Screening DBiagnosis Hamamy 2010Georgie StephenNo ratings yet
- Congenital Diaphragmatic Hernia (CDH) Information For Health ProfessionalsDocument5 pagesCongenital Diaphragmatic Hernia (CDH) Information For Health ProfessionalsMangku Liong GuanNo ratings yet
- Anembryonic PregnancyDocument6 pagesAnembryonic PregnancyElizabeth DaligdigNo ratings yet
- Prenatal Diagnosis and ScreeningDocument55 pagesPrenatal Diagnosis and ScreeningRania ZahoNo ratings yet
- Genetic Evaluation For Craniofacial ConditionsDocument21 pagesGenetic Evaluation For Craniofacial ConditionsMarcela Cano RicardoNo ratings yet
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDocument6 pagesStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNo ratings yet
- Andrologia 2019Document9 pagesAndrologia 2019mayra alejandra pinilla guerreroNo ratings yet
- Talk 8 New Biologic Agents in LN - Richard J. GlassockDocument67 pagesTalk 8 New Biologic Agents in LN - Richard J. GlassockTeodora JoghiuNo ratings yet
- Autoimmune Hemolytic AnaemiaDocument32 pagesAutoimmune Hemolytic AnaemiaJohn VinithNo ratings yet
- 2013 ACC/AHA Guidelines On The Assessment of Atherosclerotic Cardiovascular RiskDocument21 pages2013 ACC/AHA Guidelines On The Assessment of Atherosclerotic Cardiovascular RiskJohn VinithNo ratings yet
- Antinuclear Antibody SummaryDocument2 pagesAntinuclear Antibody SummaryJohn VinithNo ratings yet
- Neurology ExaminationDocument5 pagesNeurology ExaminationJohn VinithNo ratings yet
- Project Execution ProcedureDocument4 pagesProject Execution Procedurecyno2167% (3)
- Shandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23Document130 pagesShandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23mliugong94% (16)
- Yoga & Diet To Prevent DepressionDocument5 pagesYoga & Diet To Prevent DepressionDietician Mrunmayee DixitNo ratings yet
- Sakshijain75.Final ProDocument46 pagesSakshijain75.Final ProOm AherNo ratings yet
- Color Me VeganDocument272 pagesColor Me VeganBela Luísa Novo100% (1)
- Ishrae 365 2009 PDFDocument16 pagesIshrae 365 2009 PDFZeeshan HasanNo ratings yet
- (IJCST-V11I6P5) :A.E.E. El-Alfi, M. E. A. Awad, F. A. A. KhalilDocument9 pages(IJCST-V11I6P5) :A.E.E. El-Alfi, M. E. A. Awad, F. A. A. KhalilEighthSenseGroupNo ratings yet
- Understanding the Relationship Between Place and HealthDocument14 pagesUnderstanding the Relationship Between Place and HealtheNo ratings yet
- S# Isin CFI Code (As Per New ISO) Security Name Security Symbol Sector Name Security Type StatusDocument25 pagesS# Isin CFI Code (As Per New ISO) Security Name Security Symbol Sector Name Security Type StatusahmedalishNo ratings yet
- Edwards Auto 306 CharacteristicsDocument4 pagesEdwards Auto 306 CharacteristicsJuan Antonio Rubio-LaraNo ratings yet
- Pearly Co Cleared Funds ForecastDocument8 pagesPearly Co Cleared Funds ForecastPutin Phy0% (1)
- Cat Helimax 2016 Esp 1Document74 pagesCat Helimax 2016 Esp 1HKM IngenierosNo ratings yet
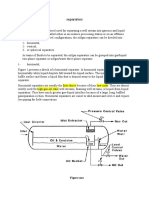
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- MIS DPCR IPCR July To December 2018 - Summary ListDocument14 pagesMIS DPCR IPCR July To December 2018 - Summary ListZyreen Kate BC100% (1)
- SP-200 Advanced PumpDocument4 pagesSP-200 Advanced PumpOsvaldo BravoNo ratings yet
- 2020 End Year 6 PenulisanDocument8 pages2020 End Year 6 PenulisanZulhillmi ZainuddinNo ratings yet
- Science Activity Sheet Quarter 4 - MELC 2 Week 2: Uses of WaterDocument13 pagesScience Activity Sheet Quarter 4 - MELC 2 Week 2: Uses of WaterShareinne TeamkNo ratings yet
- Indian Pharmacopiea 2007Document73 pagesIndian Pharmacopiea 2007Deepak ShahNo ratings yet
- Psychedelic Drugs-A New Era in Psychiatry?Document9 pagesPsychedelic Drugs-A New Era in Psychiatry?PeterNo ratings yet
- Indian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaDocument13 pagesIndian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaPranjal MaluNo ratings yet
- FarkolDocument7 pagesFarkolHasiadin LaodeNo ratings yet
- Chap 24 Econ 40Document4 pagesChap 24 Econ 40Racel DelacruzNo ratings yet
- Analysis of Drinking Water Quality Parameters (A Case Study of Hanumangarh Town)Document8 pagesAnalysis of Drinking Water Quality Parameters (A Case Study of Hanumangarh Town)Editor IJTSRDNo ratings yet
- Uber ComplaintDocument17 pagesUber ComplaintMichael TobinNo ratings yet
- Order - Judgement Query Coram WiseDocument13 pagesOrder - Judgement Query Coram Wisesatish_CJNo ratings yet
- DatasheetDocument112 pagesDatasheetStuxnetNo ratings yet
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
- Pharmaceutical Microbiology - B.pharmDocument383 pagesPharmaceutical Microbiology - B.pharmkeyurNo ratings yet
- Sprocket Asa 180Document1 pageSprocket Asa 180jhampolrosalesNo ratings yet