You might also like
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- DimenhydrinateDocument2 pagesDimenhydrinateNinoska Garcia-Ortiz100% (1)
- A Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ineffective Tissue Perfusion Secondary To Cellulitis DM Type 2Document3 pagesIneffective Tissue Perfusion Secondary To Cellulitis DM Type 2MichaelaKatrinaTrinidadNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJohn Ronald P. RamosNo ratings yet
- Pathophysiology of Congestive Heart Failure NarrativeDocument4 pagesPathophysiology of Congestive Heart Failure NarrativeAlfred BucabucaNo ratings yet
- Schematic Diagram of StrokeDocument1 pageSchematic Diagram of StrokeMaricar K. BrionesNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMara Jon Ocden CasibenNo ratings yet
- HYPERTENSION Health TeachingDocument3 pagesHYPERTENSION Health TeachingPaulo JavierNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Case Study Ugib Lower MBDocument65 pagesCase Study Ugib Lower MBQuolette Constante100% (1)
- Gynecologist Career EssayDocument4 pagesGynecologist Career Essayapi-531232390No ratings yet
- ACS PathophysiologyDocument2 pagesACS PathophysiologyFerliza OblenaNo ratings yet
- NCP AnxietyDocument1 pageNCP AnxietyUnang MagnayeNo ratings yet
- Clonidine Hydro ChlorideDocument4 pagesClonidine Hydro Chlorideapi-3797941100% (1)
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Nursing Care PlanDocument13 pagesNursing Care Planyumiko0% (1)
- Propranolol 1 PresentationDocument17 pagesPropranolol 1 Presentationapi-284092317100% (1)
- Nursing Care Plan. HypertensionDocument2 pagesNursing Care Plan. HypertensionKiara Shanelle Posadas AbrioNo ratings yet
- Drug PrilosecDocument1 pageDrug PrilosecSrkocher100% (1)
- Pathophysiology of Portal HYPERTENSION PDFDocument11 pagesPathophysiology of Portal HYPERTENSION PDFCamilo VidalNo ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
- HemodialysisDocument2 pagesHemodialysisjustin_saneNo ratings yet
- NCP For AsthmaDocument2 pagesNCP For AsthmawaadNo ratings yet
- Drug StudyDocument24 pagesDrug Studyabulan100% (1)
- Ineffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.Document6 pagesIneffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.SAROL, RYAN CHRISTIAN B.No ratings yet
- NCPDocument3 pagesNCPErica Denice CastilloNo ratings yet
- CASE STUDY PheumoniaDocument5 pagesCASE STUDY PheumoniaEdelweiss Marie CayetanoNo ratings yet
- 005LEU11EDocument4 pages005LEU11ELiaWahyuniNo ratings yet
- Subjective: "Sumikip Ang Dibdib Ko at Hindi Ako Makahinga NG Maayos" As IndependentDocument2 pagesSubjective: "Sumikip Ang Dibdib Ko at Hindi Ako Makahinga NG Maayos" As IndependentCorinneNo ratings yet
- Hypertension Pathophysiology and Treatment PDFDocument6 pagesHypertension Pathophysiology and Treatment PDFBella TogasNo ratings yet
- Levemir Product Insert PDFDocument11 pagesLevemir Product Insert PDFDegee O. GonzalesNo ratings yet
- Betahistine Drug InfoDocument3 pagesBetahistine Drug InfoAshish KarnNo ratings yet
- Nursing Care Plans For Activity IntoleranceDocument4 pagesNursing Care Plans For Activity IntolerancethebigtwirpNo ratings yet
- Infective Endocarditis CaseDocument3 pagesInfective Endocarditis CaseMershen GaniaNo ratings yet
- Fludrocortisone (Florinef)Document17 pagesFludrocortisone (Florinef)passer byNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJanina Patricia BuddleNo ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologyBeRnAlieNo ratings yet
- COLCHICINE pptx1800128929Document15 pagesCOLCHICINE pptx1800128929April Mergelle LapuzNo ratings yet
- ESRD PathophysiologyDocument2 pagesESRD Pathophysiologynursing concept mapsNo ratings yet
- Discharge PlanDocument1 pageDischarge PlanBernalene SyNo ratings yet
- Drug Study ColestipolDocument3 pagesDrug Study ColestipolAbby AngNo ratings yet
- NCP DM and HCVDDocument3 pagesNCP DM and HCVDMAYBELINE OBAOB100% (1)
- Generic Brand Class Therapeutic Pharmacologic Dosage: PPD's Better Pharmacy Drug Hand Book 9 Edition 2009Document4 pagesGeneric Brand Class Therapeutic Pharmacologic Dosage: PPD's Better Pharmacy Drug Hand Book 9 Edition 2009Crystal Queen MarquezNo ratings yet
- Week 3. COURSE TASK - Acute PancreatitisDocument3 pagesWeek 3. COURSE TASK - Acute PancreatitisqwertNo ratings yet
- Case AnalysisDocument25 pagesCase AnalysisGerly LagutingNo ratings yet
- Aspirin Drug StudyDocument3 pagesAspirin Drug StudyIRISH CACAYANNo ratings yet
- Drug Study FinalDocument6 pagesDrug Study FinalJade HemmingsNo ratings yet
- Tatz Pa ToolDocument23 pagesTatz Pa Toolian_mendoza_3No ratings yet
- Imbalnce Nutrition Less Than Body RequirementsDocument3 pagesImbalnce Nutrition Less Than Body RequirementselheezaNo ratings yet
- Nursing Process NUTRITIONDocument82 pagesNursing Process NUTRITIONNoci M. FrenkNo ratings yet
- AppendectomyDocument35 pagesAppendectomyleighjagNo ratings yet
- TherablocDocument3 pagesTherablocianecunar100% (2)
- Risk For Bleeding - Cirrhosis NCPDocument2 pagesRisk For Bleeding - Cirrhosis NCPPaula AbadNo ratings yet
- Osteosarcoma-Ana and PhysiologyDocument4 pagesOsteosarcoma-Ana and PhysiologyNeirfla WassabiNo ratings yet
- Drug Study EditedDocument5 pagesDrug Study EditedfabtaciousVeelaNo ratings yet
- HYPERTENSION INTERVENTION PLAN 1 FinalDocument6 pagesHYPERTENSION INTERVENTION PLAN 1 FinalKenrick Espiritu BajaoNo ratings yet
- American Heart Association Acls Post Test AnswersDocument4 pagesAmerican Heart Association Acls Post Test AnswersArun Jude Alphonse0% (9)
- General Science Ebook 1 Jagran JoshDocument136 pagesGeneral Science Ebook 1 Jagran JoshCentral Province Online Publishers50% (2)
- Scientific Survey of The Yogic PosesDocument66 pagesScientific Survey of The Yogic PosesSnehal Kale100% (1)
- Peel 1996 - Cardiopulmonary System and Movement DysfunctionDocument8 pagesPeel 1996 - Cardiopulmonary System and Movement DysfunctionBeto ZamunérNo ratings yet
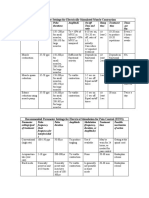
- Parameter Settings For Electrically Stimulated Muscle ContractionDocument3 pagesParameter Settings For Electrically Stimulated Muscle Contractionpallen100% (5)
- Quantum Healing CodesDocument59 pagesQuantum Healing CodesSIMONA-LUMINITA96% (28)
- (Uace) Abe Holy Cross LV Jinja 07th 10 2023Document20 pages(Uace) Abe Holy Cross LV Jinja 07th 10 2023bridgous3No ratings yet
- S11 12LT IIIaj 17Document3 pagesS11 12LT IIIaj 17Evangelene Esquillo SanaNo ratings yet
- Calcium Channel BlockersDocument35 pagesCalcium Channel BlockersSufyan MirzaNo ratings yet
- HEART MURMURS by NISHDocument41 pagesHEART MURMURS by NISHurtikikeNo ratings yet
- AHA Card CombinedDocument2 pagesAHA Card CombinedAdrian Gutierrez NajeraNo ratings yet
- Heal Yourself Naturally PaidalajinDocument219 pagesHeal Yourself Naturally Paidalajinluis alejandro osorio100% (7)
- HypertensionDocument36 pagesHypertensionRECEPTION AND DIAGNOSTIC CENTER RDC MEDICAL SECTIONNo ratings yet
- Managing Palpitations and Arrhythmias During Pregnancy: Dawn L Adamson, Catherine Nelson-PiercyDocument7 pagesManaging Palpitations and Arrhythmias During Pregnancy: Dawn L Adamson, Catherine Nelson-PiercyFlo ArdyansyahNo ratings yet
- Differential Response of Central Blood Pressure To Isometric and Isotonic ExerciseDocument5 pagesDifferential Response of Central Blood Pressure To Isometric and Isotonic ExerciseTAINAH DE PAULANo ratings yet
- Chest To Abdomen AssessmentDocument16 pagesChest To Abdomen AssessmentLuzel Lapuz100% (1)
- TnpscdoDocument38 pagesTnpscdoJeshiNo ratings yet
- Anatomy and SssDocument9 pagesAnatomy and SssAia JavierNo ratings yet
- Conduction System of The Heart PPT 2Document12 pagesConduction System of The Heart PPT 2leigh angelaNo ratings yet
- Normal Electrocardiogram: Lucia Kris Dinarti Cardiology Department Faculty of Medicine GMUDocument21 pagesNormal Electrocardiogram: Lucia Kris Dinarti Cardiology Department Faculty of Medicine GMUMuhammad Ricky RamadhianNo ratings yet
- CardiotocographyDocument46 pagesCardiotocographyElisabeth F. OjhaNo ratings yet
- Activity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020Document10 pagesActivity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020RJ TacataNo ratings yet
- Thesis Statement Competitive SwimmingDocument7 pagesThesis Statement Competitive Swimminggof1mytamev2100% (2)
- Pulmonary Atresia With Intact Ventricular Septum: PA/IVSDocument36 pagesPulmonary Atresia With Intact Ventricular Septum: PA/IVSRedmond P. Burke MD100% (1)
- Frank Clark AutopsyDocument8 pagesFrank Clark AutopsyK Fine100% (1)
- Lesson 10 Long Term Effects of ExerciseDocument11 pagesLesson 10 Long Term Effects of ExerciseMaliha RiazNo ratings yet
- Types of ExerciseDocument6 pagesTypes of ExerciseReid AbajonNo ratings yet
- Previous Question Paper 1 CardiologyDocument5 pagesPrevious Question Paper 1 CardiologyDeepthi DNo ratings yet
- Finnal Lab Anatomi - A - Annisa Dg. PatapaDocument7 pagesFinnal Lab Anatomi - A - Annisa Dg. PatapaZulhajja Nur08No ratings yet
- Anatomy Question BankDocument41 pagesAnatomy Question Bankavantika rajeev100% (1)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (3)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (351)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (82)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (411)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesFrom EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthFrom EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthRating: 4 out of 5 stars4/5 (7)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Molecules of Emotion: Why You Feel the Way You FeelFrom EverandMolecules of Emotion: Why You Feel the Way You FeelRating: 4 out of 5 stars4/5 (128)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)