You might also like
- TTIKDocument50 pagesTTIKSparkling PinkNo ratings yet
- 5.daftar Pustaka Ramsay Hunt SyndromeDocument3 pages5.daftar Pustaka Ramsay Hunt SyndromeSparkling PinkNo ratings yet
- Dyslexia (From Yale)Document4 pagesDyslexia (From Yale)Sparkling PinkNo ratings yet
- Follow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKDocument2 pagesFollow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKSparkling PinkNo ratings yet
- Myelopathy (Spine)Document34 pagesMyelopathy (Spine)Sparkling PinkNo ratings yet
- Bruits of The Head and Neck (Wildchild)Document6 pagesBruits of The Head and Neck (Wildchild)Sparkling PinkNo ratings yet
- Perdarahan SubaraknoidDocument7 pagesPerdarahan SubaraknoidJessica SilaenNo ratings yet
- Hipertrigliseridemia in PregnancyDocument5 pagesHipertrigliseridemia in PregnancySparkling PinkNo ratings yet
- ALS Amyotrophic Lateral Sclerosis Literature Review 1 - 14Document11 pagesALS Amyotrophic Lateral Sclerosis Literature Review 1 - 14Sparkling PinkNo ratings yet
- Jadwal Jaga Observer April 2016Document2 pagesJadwal Jaga Observer April 2016Sparkling PinkNo ratings yet
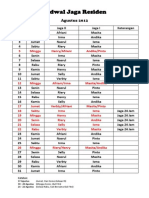
- On Call Schedule, Night Shift Schedule, Hospital, Residency Program, Neurology, Life, August 2012. Tentative Program.Document2 pagesOn Call Schedule, Night Shift Schedule, Hospital, Residency Program, Neurology, Life, August 2012. Tentative Program.Sparkling PinkNo ratings yet
- Diabetes Mellitus in PregnancyDocument12 pagesDiabetes Mellitus in PregnancyFadila R. Lubis LubisNo ratings yet
- On-Call Schedule: August 2012Document2 pagesOn-Call Schedule: August 2012Sparkling PinkNo ratings yet
- Daftar Pustaka ALSDocument2 pagesDaftar Pustaka ALSSparkling PinkNo ratings yet
- Effects of Vitamin E On Stroke SubtypesDocument17 pagesEffects of Vitamin E On Stroke SubtypesSparkling PinkNo ratings yet
- Alcohol and Acute Ischemic Stroke OnsetDocument30 pagesAlcohol and Acute Ischemic Stroke OnsetSparkling PinkNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Amyotrophic Lateral SclerosisDocument58 pagesAmyotrophic Lateral SclerosisAathi PathmanathanNo ratings yet
- Motor Neuron DiseaseDocument8 pagesMotor Neuron DiseaseyigoNo ratings yet
- Alsreport 2005Document359 pagesAlsreport 2005David GritschNo ratings yet
- Charway-Felli - Spinal Cord Disorders - Epidemiology and ClassificationDocument33 pagesCharway-Felli - Spinal Cord Disorders - Epidemiology and Classificationgem estsy100% (1)
- Drosophila Melanogaster Models of Motor Neuron Disease 2013 (Edited by Ruben Cauchi)Document239 pagesDrosophila Melanogaster Models of Motor Neuron Disease 2013 (Edited by Ruben Cauchi)Dr.Gill_Grissom100% (1)
- Sun Maiden PlusDocument6 pagesSun Maiden PlusJesus HernandezNo ratings yet
- ALS A Revision of The El Escorial Criteria 2015Document2 pagesALS A Revision of The El Escorial Criteria 2015Ahmad ShokryNo ratings yet
- Clinical Features of Amyotrophic Lateral Sclerosis and Other Forms of Motor Neuron Disease UpToDate PDFDocument21 pagesClinical Features of Amyotrophic Lateral Sclerosis and Other Forms of Motor Neuron Disease UpToDate PDFThái BảoNo ratings yet
- 02D Progressive Muscular AtrophyDocument12 pages02D Progressive Muscular AtrophyMonica CusniriucNo ratings yet
- UntitledDocument369 pagesUntitledveerraju tvNo ratings yet
- Feldman. Esclerosis Lateral Amiotrófica, Artículo de The Lancet 2022 - EngDocument18 pagesFeldman. Esclerosis Lateral Amiotrófica, Artículo de The Lancet 2022 - EngAndrei LahoreNo ratings yet
- Adams and Victor's - Principles of Neurology-Pages-1073-1137 PDFDocument65 pagesAdams and Victor's - Principles of Neurology-Pages-1073-1137 PDFDin100% (2)
- Clinical Spectrum of Motor Neuron Disorders.8Document21 pagesClinical Spectrum of Motor Neuron Disorders.8Anonymous vnv6QFNo ratings yet
- Pinto 2019Document12 pagesPinto 2019Fábio VinholyNo ratings yet