You might also like
- Siblings With Hepatosplenomegaly and Lipoprotein Lipase DeficiencyDocument2 pagesSiblings With Hepatosplenomegaly and Lipoprotein Lipase DeficiencyfirdakusumaputriNo ratings yet
- Pregnancy PDFDocument4 pagesPregnancy PDFEileen MateoNo ratings yet
- Acute Fatty Liver Versus HELLPDocument44 pagesAcute Fatty Liver Versus HELLPrainmaker77771121100% (1)
- Hypertriglyceridemia (962) Paper FinalDocument5 pagesHypertriglyceridemia (962) Paper FinalAkhilaNo ratings yet
- Jaundiceandpregnancy JIACMDocument7 pagesJaundiceandpregnancy JIACMHaekal HafizhNo ratings yet
- The Hellp Syndrome - A Therapeutic ChallengeDocument41 pagesThe Hellp Syndrome - A Therapeutic Challengeد. أحمد عبد الباسطNo ratings yet
- Thrombocytopenia Pocket GuideDocument8 pagesThrombocytopenia Pocket GuideAnnisaValentKhanNo ratings yet
- Postgrad Med J 2010 Mackillop 160 4Document6 pagesPostgrad Med J 2010 Mackillop 160 4Gonzalo MendozaNo ratings yet
- HELLP SyndromeDocument5 pagesHELLP SyndromeAhmed ALiNo ratings yet
- 1 s2.0 S237606052100122X MainDocument3 pages1 s2.0 S237606052100122X MainOana MihaelaNo ratings yet
- Hypertension IN PregnanciesDocument36 pagesHypertension IN Pregnanciesdaniel mitikuNo ratings yet
- Biochemical Changes in PregnancyDocument6 pagesBiochemical Changes in PregnancyDr.Aaisha Mohammed Al BalushiNo ratings yet
- Maternal Fetal PhysiologyDocument28 pagesMaternal Fetal PhysiologyHaadi AliNo ratings yet
- Backgroun 1Document3 pagesBackgroun 1Idi Nagan RayaNo ratings yet
- D. Huda Liver Diseases and Pregnancy-1 (Muhadharaty)Document34 pagesD. Huda Liver Diseases and Pregnancy-1 (Muhadharaty)Ihab MahmoodNo ratings yet
- Hyperemesis Gravidarum: by Dr. Abdel Magid M.Ahmed Nov. 2015Document16 pagesHyperemesis Gravidarum: by Dr. Abdel Magid M.Ahmed Nov. 2015Ibrahim JameelallaNo ratings yet
- Fatty Liver in Pregnancy - StatPearls - NCBI BookshelfDocument6 pagesFatty Liver in Pregnancy - StatPearls - NCBI BookshelfAndres Pimentel AlvarezNo ratings yet
- Preeclampsia and EclampsiaDocument24 pagesPreeclampsia and EclampsiaAngel Marie TeNo ratings yet
- Management of Jaundice in Pregnancy 2010Document7 pagesManagement of Jaundice in Pregnancy 2010Dhisa Zainita HabsariNo ratings yet
- Acute Fatty Liver of Pregnancy: A Case ReportDocument0 pagesAcute Fatty Liver of Pregnancy: A Case ReportnajmulNo ratings yet
- HypertriglyceridemiaDocument8 pagesHypertriglyceridemiaNaila KhanNo ratings yet
- Liver Function TesDocument58 pagesLiver Function TesnoffrizalNo ratings yet
- Hellp SyndromeDocument2 pagesHellp SyndromeAnonymous EA9uILwJ08No ratings yet
- Acute Fatty Liver With PregnancyDocument50 pagesAcute Fatty Liver With PregnancyDr. mohammed100% (1)
- Liverdiseaseinpregnancy 2Document40 pagesLiverdiseaseinpregnancy 2Fadil HidayatNo ratings yet
- Management of Pregnancy JaundiceDocument28 pagesManagement of Pregnancy JaundiceShailani Thakur100% (1)
- Kuthiroly2021 Article LipoproteinLipaseDeficiencyDocument7 pagesKuthiroly2021 Article LipoproteinLipaseDeficiencybrajendra singhNo ratings yet
- Adiponectin: Chien-Wen Chou MD. Endocrinology & Metabolism Division Chi-Mei Medical Center 22 April 2005Document18 pagesAdiponectin: Chien-Wen Chou MD. Endocrinology & Metabolism Division Chi-Mei Medical Center 22 April 2005Efi RamadhaniNo ratings yet
- Fatty Liver Disease of Cattle - Metabolic Disorders - MSD Veterinary ManualDocument7 pagesFatty Liver Disease of Cattle - Metabolic Disorders - MSD Veterinary ManualsayemkhanmarwatNo ratings yet
- Diagnosis of Ectopic PregnancyDocument17 pagesDiagnosis of Ectopic PregnancykushalNo ratings yet
- Metabolic SyndromeDocument55 pagesMetabolic SyndromeAakash BalasubramanianNo ratings yet
- Biochemistry-1 - 1Document13 pagesBiochemistry-1 - 1khaledNo ratings yet
- Acute Fatty Liver of Pregnancy: Letter To EditorDocument2 pagesAcute Fatty Liver of Pregnancy: Letter To EditorsaryindrianyNo ratings yet
- DR - Kavitha NagarajanDocument32 pagesDR - Kavitha NagarajanKavitha NagarajanNo ratings yet
- 17 Falla Renal Aguda en La GestacionDocument4 pages17 Falla Renal Aguda en La GestacionjuanNo ratings yet
- Autoimmune HepatitisDocument3 pagesAutoimmune HepatitisMohammed FaragNo ratings yet
- Carbohydrates Metabolism and Diabetes MellitusDocument63 pagesCarbohydrates Metabolism and Diabetes Mellitusapi-19641337No ratings yet
- Liver Disease in Pregnancy: J. Eileen HayDocument10 pagesLiver Disease in Pregnancy: J. Eileen HayNirmala PudakalkattiNo ratings yet
- Early OnsetDocument6 pagesEarly Onsetiaset123No ratings yet
- Pseudohyponatremia Nejm CpsDocument7 pagesPseudohyponatremia Nejm CpshoneyworksNo ratings yet
- Diagosis and Management of Preeclampsia: Journal Presentation Ayu Wulan Anggreni 030.05.046Document17 pagesDiagosis and Management of Preeclampsia: Journal Presentation Ayu Wulan Anggreni 030.05.046Ayu Rahmi AMyNo ratings yet
- HEGDocument23 pagesHEGSamer SaoumaNo ratings yet
- Maternal and Perinatal Outcome in Severe Pregnancy Related Liver DiseasesDocument5 pagesMaternal and Perinatal Outcome in Severe Pregnancy Related Liver Diseasesadrip234No ratings yet
- Gestosis MergedDocument141 pagesGestosis MergedRamNo ratings yet
- Hellp PDFDocument2 pagesHellp PDFSteven Tapia VillacísNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- The Hellp Syndrome: DR Dohbit Sama Obs-Gyn H.G.O.P.Y - YaoundeDocument19 pagesThe Hellp Syndrome: DR Dohbit Sama Obs-Gyn H.G.O.P.Y - Yaoundemusinguzi albertNo ratings yet
- Patel 2020Document31 pagesPatel 2020larissa brandaliseNo ratings yet
- Fatty Liver Disease of CattleDocument4 pagesFatty Liver Disease of Cattleابراهيم القويعىNo ratings yet
- Hellp SyndromeDocument41 pagesHellp SyndromeDiena HarisahNo ratings yet
- Jaundice in PregnancyDocument13 pagesJaundice in PregnancyAnonymous mvNUtwidNo ratings yet
- Biochem QuestionsDocument15 pagesBiochem QuestionsSamantha SerraoNo ratings yet
- Presentation - LipoproteinDocument31 pagesPresentation - Lipoproteinrahulshrmaa2222No ratings yet
- HELLPSyndromeDocument40 pagesHELLPSyndromeDaniela IlieNo ratings yet
- Normal Protein Diet and L-Ornithine-L-Aspartate For Hepatic EncephalopathyDocument4 pagesNormal Protein Diet and L-Ornithine-L-Aspartate For Hepatic EncephalopathyElisa SalakayNo ratings yet
- Chronic Renal Failure During PregnancyDocument42 pagesChronic Renal Failure During PregnancyvincentsharonNo ratings yet
- Lipodistrofia FamiliarDocument4 pagesLipodistrofia FamiliarKaren Magalí CruzNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Follow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKDocument2 pagesFollow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKSparkling PinkNo ratings yet
- 5.daftar Pustaka Ramsay Hunt SyndromeDocument3 pages5.daftar Pustaka Ramsay Hunt SyndromeSparkling PinkNo ratings yet
- Myelopathy (Spine)Document34 pagesMyelopathy (Spine)Sparkling PinkNo ratings yet
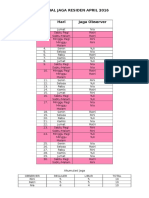
- Jadwal Jaga Observer April 2016Document2 pagesJadwal Jaga Observer April 2016Sparkling PinkNo ratings yet
- On-Call Schedule: August 2012Document2 pagesOn-Call Schedule: August 2012Sparkling PinkNo ratings yet
- Guideline On Behavior Guidance For The Pediatric Dental Patient PDFDocument13 pagesGuideline On Behavior Guidance For The Pediatric Dental Patient PDFDaniel Alberto Jimenez JarquinNo ratings yet
- Test QuestionsDocument2 pagesTest QuestionsLucille E. TesadoNo ratings yet
- Independent Practice Issues and Independent Midwifery Nursing PRACTIONERDocument14 pagesIndependent Practice Issues and Independent Midwifery Nursing PRACTIONERKrini Tandel100% (4)
- Peritoneal DialysisDocument3 pagesPeritoneal DialysisGoh Kek BoonNo ratings yet
- Lesson Plan On Procedure of Bed BathDocument9 pagesLesson Plan On Procedure of Bed Bathchinchu64% (14)
- Osce PDFDocument228 pagesOsce PDFOnur Temizsoylu100% (1)
- Pathology - 24 Breast PathologyDocument9 pagesPathology - 24 Breast PathologyNicole WilliamNo ratings yet
- 9.a Nationwide Evidence-Based Study of Factors Associated With Hospitalizations Due To Unintentional Poisoning and Poisoning Mortality in TaiwanDocument8 pages9.a Nationwide Evidence-Based Study of Factors Associated With Hospitalizations Due To Unintentional Poisoning and Poisoning Mortality in Taiwan小葉No ratings yet
- Winchester Anesthesia Ebook PDFDocument59 pagesWinchester Anesthesia Ebook PDFAdi Nugroho Melyana100% (1)
- DiabetesDocument38 pagesDiabetesaquakumbh75% (4)
- Daftar Pustaka: Medicine. 7 Ed. Churchill Livingstone: EdinburgDocument3 pagesDaftar Pustaka: Medicine. 7 Ed. Churchill Livingstone: EdinburgseptinaNo ratings yet
- Images of Nurses in MediaDocument8 pagesImages of Nurses in MediaRufus Raj50% (2)
- 78 24 100324ExE13Document160 pages78 24 100324ExE13Himanshu PurohitNo ratings yet
- Non-Bone Graft Associated Regenerative Periodontal TherapyDocument80 pagesNon-Bone Graft Associated Regenerative Periodontal TherapyGorremuchu Srinivas0% (1)
- VHA Handbook 1100Document81 pagesVHA Handbook 1100Ratna fatimahNo ratings yet
- Basantis ResumeDocument2 pagesBasantis ResumesurajitnykNo ratings yet
- Cold InjuryDocument34 pagesCold Injurydassdeepak69100% (1)
- Hypertension Prepost Test - Answer KeyDocument3 pagesHypertension Prepost Test - Answer Keyapi-247079964100% (1)
- Functional Evaluation of Lumbar Spinal Stenosis Treated With Conservative Treatment Retrospective StudyDocument5 pagesFunctional Evaluation of Lumbar Spinal Stenosis Treated With Conservative Treatment Retrospective StudyAzmi FarhadiNo ratings yet
- Anestesia Gow Gates 2Document7 pagesAnestesia Gow Gates 2Marriano DarinoNo ratings yet
- Test Bank Abnormal Psychology 1st Edition Butcher PDFDocument60 pagesTest Bank Abnormal Psychology 1st Edition Butcher PDFRaiza BettinaNo ratings yet
- Interpretation of Lab TestsDocument29 pagesInterpretation of Lab TestsRitesh Singh100% (6)
- Medical NotesDocument4 pagesMedical NotesRain CastillaNo ratings yet
- 1st Sem Sport Science Assignment ContentDocument9 pages1st Sem Sport Science Assignment ContentKobasen LimNo ratings yet
- Brain Development of Children From 0 To 6 Years How The Brain LearnsDocument1 pageBrain Development of Children From 0 To 6 Years How The Brain Learnssyarifah wardah el hilwaNo ratings yet
- Lattice DegenerationDocument2 pagesLattice DegenerationamandaNo ratings yet
- Smoking CessationDocument48 pagesSmoking CessationSingey LhendupNo ratings yet
- Bronchiolitis Rs V Current Concepts 2009Document75 pagesBronchiolitis Rs V Current Concepts 2009adnan.engineer17049No ratings yet
- Prof Qaisar Khan TrialsDocument56 pagesProf Qaisar Khan TrialsAsim NajamNo ratings yet
- Activity 3 Case Scenario GcsDocument3 pagesActivity 3 Case Scenario GcsDfatsbsNo ratings yet