You might also like
- Home Abdomen Breast Cardiovascular Chest Head Neck MusculoskeletalDocument18 pagesHome Abdomen Breast Cardiovascular Chest Head Neck Musculoskeletalririn selagalasNo ratings yet
- The Radiology Assistant MyelopathyDocument3 pagesThe Radiology Assistant MyelopathyMarisol DíazNo ratings yet
- Multiple SclerosisDocument4 pagesMultiple SclerosisMarwan M.No ratings yet
- Ni 09039Document8 pagesNi 09039Tomi NugrahaNo ratings yet
- Clinically Isolated Syndrome (CIS)Document12 pagesClinically Isolated Syndrome (CIS)Dorin Cristian AntalNo ratings yet
- c4f - Multiple SclerosisDocument240 pagesc4f - Multiple Sclerosisstewpitt2No ratings yet
- Evaluation and Diagnosis of Multiple Sclerosis in Adults - UpToDateDocument45 pagesEvaluation and Diagnosis of Multiple Sclerosis in Adults - UpToDatespritdummyNo ratings yet
- 1.1 Overview: Brain Tissues ClassificationDocument66 pages1.1 Overview: Brain Tissues ClassificationashokkumarNo ratings yet
- Multipel Sklerosis Tumefaktif: Laporan KasusDocument7 pagesMultipel Sklerosis Tumefaktif: Laporan KasusAndi khamisrahNo ratings yet
- MS FileDocument8 pagesMS FileFARAH MOHAMMEDNo ratings yet
- Draw Ang Label The Major Parts of The Nervous System. (Brain and Spinal Cord)Document9 pagesDraw Ang Label The Major Parts of The Nervous System. (Brain and Spinal Cord)ShainaChescaEvansNo ratings yet
- Print 2Document13 pagesPrint 2jtd9h2xp5hNo ratings yet
- Multiple SclerosisDocument6 pagesMultiple SclerosisMBENOYNo ratings yet
- Cranial Nerve DisordersDocument218 pagesCranial Nerve DisordersRem AlfelorNo ratings yet
- Pediatric Spine MRI: Occult Spinal DysraphismsDocument5 pagesPediatric Spine MRI: Occult Spinal DysraphismsSilma FarrahaNo ratings yet
- Cervical SpondylosisDocument10 pagesCervical Spondylosistaufiq duppa duppaaNo ratings yet
- Multiple SclerosisDocument8 pagesMultiple SclerosisNader Smadi100% (1)
- Nervous System DiseasesDocument16 pagesNervous System DiseasesShahzad ShameemNo ratings yet
- Brain & S. C. Tumors, Aneurysm, AVM, Trigeminal Neuralgia, Bell's PalsyDocument15 pagesBrain & S. C. Tumors, Aneurysm, AVM, Trigeminal Neuralgia, Bell's PalsypertinenteNo ratings yet
- Cervical MyelopathyDocument7 pagesCervical Myelopathybmahmood1No ratings yet
- 13 Demyelinating DiseaseDocument8 pages13 Demyelinating DiseasemgvbNo ratings yet
- Spinal Muscular AtrophyDocument18 pagesSpinal Muscular AtrophyJelica LlanilloNo ratings yet
- Imaging of Musculoskeletal SystemDocument53 pagesImaging of Musculoskeletal SystemSara ManzoorNo ratings yet
- Haramaya University: College of Health and Medical Science Department of Midwifery NeurologyDocument54 pagesHaramaya University: College of Health and Medical Science Department of Midwifery NeurologyMerwan KemalNo ratings yet
- Recit NeuroDocument11 pagesRecit Neuroliii jzjxjsNo ratings yet
- Spinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيDocument33 pagesSpinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيMohammad BelbahaithNo ratings yet
- Surgical Management of Cervical Myelopathy: Clinical EvaulationDocument10 pagesSurgical Management of Cervical Myelopathy: Clinical EvaulationBaharudin Yusuf RamadhaniNo ratings yet
- طب باطني (نظري) م8Document4 pagesطب باطني (نظري) م8asalla.fayyad.rdNo ratings yet
- A Quick Guide For Neuroimaging of Common Dementias Seen in Clinical PracticeDocument8 pagesA Quick Guide For Neuroimaging of Common Dementias Seen in Clinical PracticeAndika ResaNo ratings yet
- Multiple SclerosisDocument4 pagesMultiple SclerosisnasibdinNo ratings yet
- Motor Neurone Disease PDFDocument4 pagesMotor Neurone Disease PDFTONY GO AWAYNo ratings yet
- Menu: Print ShareDocument37 pagesMenu: Print ShareAndreea CimpoiNo ratings yet
- Acute Transverse MyelitisDocument3 pagesAcute Transverse MyelitisCS NarayananNo ratings yet
- Tumors of The Nervous SystemDocument6 pagesTumors of The Nervous SystemRituNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document8 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)octiaraesyaNo ratings yet
- Myelopathy But Normal MRI-What's Next?, JNNP 2008Document14 pagesMyelopathy But Normal MRI-What's Next?, JNNP 2008NEuRoLoGisT CoFFeeCuP100% (3)
- SDL 8 Intracranial Space Occupying LesionDocument5 pagesSDL 8 Intracranial Space Occupying LesionJonathan YeohNo ratings yet
- Variants of Multiple Sclerosis: Jack H. Simon,, B.K. Kleinschmidt-DemastersDocument14 pagesVariants of Multiple Sclerosis: Jack H. Simon,, B.K. Kleinschmidt-DemastersNoor HadiNo ratings yet
- Medulla Spinalis: (Spinal Cord)Document37 pagesMedulla Spinalis: (Spinal Cord)Dek SriNo ratings yet
- Ms PresentationDocument9 pagesMs Presentationapi-262174667No ratings yet
- Multiple SclerosisDocument17 pagesMultiple SclerosisSyiozz PoongundranNo ratings yet
- Bilateral Acquired Ptosis, An Unusual Presentation of A Cerebral Arteriovenous MalformationDocument3 pagesBilateral Acquired Ptosis, An Unusual Presentation of A Cerebral Arteriovenous MalformationRin4lNo ratings yet
- Cervical InjuryDocument9 pagesCervical Injurypmahi8854No ratings yet
- Imagenes en MielopatiaDocument23 pagesImagenes en MielopatiaYanina Pérez de VillarrealNo ratings yet
- Motor Neurone Disease ThesisDocument2 pagesMotor Neurone Disease ThesisParth Vijay SinghNo ratings yet
- Ref E.M.Document29 pagesRef E.M.simoneNo ratings yet
- Motor Neuron DiseaseDocument7 pagesMotor Neuron DiseasegeraldineongNo ratings yet
- Slkdmsalkdmla Sa NlasDocument12 pagesSlkdmsalkdmla Sa NlasjdjhdNo ratings yet
- Approach To A Patient With ParaplegiaDocument31 pagesApproach To A Patient With ParaplegiaFaisal Qureshi75% (4)
- Muscular DystoniaDocument20 pagesMuscular Dystoniarudresh singhNo ratings yet
- Location, Length, and Enhancement: Systematic Approach To Differentiating Intramedullary Spinal Cord LesionsDocument16 pagesLocation, Length, and Enhancement: Systematic Approach To Differentiating Intramedullary Spinal Cord LesionsdenisNo ratings yet
- Neuromyelitis Optica Spectrum Disorders.15Document33 pagesNeuromyelitis Optica Spectrum Disorders.15Marco Macavilca CruzNo ratings yet
- Gangguan Saraf KranialDocument30 pagesGangguan Saraf KranialWisnu Surya WardhanaNo ratings yet
- Case Study - Multiple SclerosisDocument3 pagesCase Study - Multiple SclerosisRachel KoenigsonNo ratings yet
- Spine: Imaging TechniquesDocument29 pagesSpine: Imaging TechniquesBrian LucasNo ratings yet
- Inflammatory Diseases of The CNSDocument21 pagesInflammatory Diseases of The CNSMalueth AnguiNo ratings yet
- Differences Between Myelopathy and RadiculopathyDocument4 pagesDifferences Between Myelopathy and RadiculopathyWidiana KosasihNo ratings yet
- White Matter DiseaseDocument55 pagesWhite Matter DiseasePeacemongerNo ratings yet
- Cerebellar LesionsDocument3 pagesCerebellar LesionsAnonymous GlBfciNo ratings yet
- TTIKDocument50 pagesTTIKSparkling PinkNo ratings yet
- 5.daftar Pustaka Ramsay Hunt SyndromeDocument3 pages5.daftar Pustaka Ramsay Hunt SyndromeSparkling PinkNo ratings yet
- Dyslexia (From Yale)Document4 pagesDyslexia (From Yale)Sparkling PinkNo ratings yet
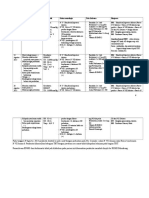
- Follow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKDocument2 pagesFollow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKSparkling PinkNo ratings yet
- Bruits of The Head and Neck (Wildchild)Document6 pagesBruits of The Head and Neck (Wildchild)Sparkling PinkNo ratings yet
- Perdarahan SubaraknoidDocument7 pagesPerdarahan SubaraknoidJessica SilaenNo ratings yet
- ALS Amyotrophic Lateral Sclerosis Literature Review 1 - 14Document11 pagesALS Amyotrophic Lateral Sclerosis Literature Review 1 - 14Sparkling PinkNo ratings yet
- Hipertrigliseridemia in PregnancyDocument5 pagesHipertrigliseridemia in PregnancySparkling PinkNo ratings yet
- Penda Hulu AnDocument4 pagesPenda Hulu AnSparkling PinkNo ratings yet
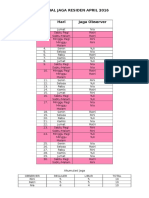
- Jadwal Jaga Observer April 2016Document2 pagesJadwal Jaga Observer April 2016Sparkling PinkNo ratings yet
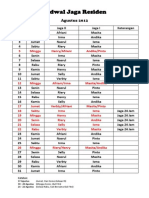
- On Call Schedule, Night Shift Schedule, Hospital, Residency Program, Neurology, Life, August 2012. Tentative Program.Document2 pagesOn Call Schedule, Night Shift Schedule, Hospital, Residency Program, Neurology, Life, August 2012. Tentative Program.Sparkling PinkNo ratings yet
- Diabetes Mellitus in PregnancyDocument12 pagesDiabetes Mellitus in PregnancyFadila R. Lubis LubisNo ratings yet
- On-Call Schedule: August 2012Document2 pagesOn-Call Schedule: August 2012Sparkling PinkNo ratings yet
- Daftar Pustaka ALSDocument2 pagesDaftar Pustaka ALSSparkling PinkNo ratings yet
- Effects of Vitamin E On Stroke SubtypesDocument17 pagesEffects of Vitamin E On Stroke SubtypesSparkling PinkNo ratings yet
- Alcohol and Acute Ischemic Stroke OnsetDocument30 pagesAlcohol and Acute Ischemic Stroke OnsetSparkling PinkNo ratings yet
- Material Safety Data Sheet: Product and Company Identification 1Document11 pagesMaterial Safety Data Sheet: Product and Company Identification 1Simon WijayaNo ratings yet
- Counterfeit DrugsDocument2 pagesCounterfeit DrugsfreeBlidaman0967% (3)
- Agenda: DAY ONE: Wednesday, March 3, 2021Document8 pagesAgenda: DAY ONE: Wednesday, March 3, 2021nsk79inNo ratings yet
- FijiTimes - May 25 2012Document48 pagesFijiTimes - May 25 2012fijitimescanadaNo ratings yet
- Perfect 2015Document6 pagesPerfect 2015windaNo ratings yet
- Other Relevant Social Concerns: Lesson 8Document18 pagesOther Relevant Social Concerns: Lesson 8Jyell CabigasNo ratings yet
- NCCN Antiemesis Guideline 2018 v3 PDFDocument68 pagesNCCN Antiemesis Guideline 2018 v3 PDFholdonpainendsNo ratings yet
- Health and Safety Environmental ManagementakistanDocument40 pagesHealth and Safety Environmental ManagementakistanAminullah01No ratings yet
- K102 Referencing FAQs 21JDocument5 pagesK102 Referencing FAQs 21JpaulNo ratings yet
- Acceptance LetterDocument40 pagesAcceptance LetterDonald IbonaNo ratings yet
- 1 SMDocument10 pages1 SMsatuA keslingNo ratings yet
- Disaster Management at Site and at HospitalDocument21 pagesDisaster Management at Site and at HospitalAlmasNo ratings yet
- Career Map AssignmentDocument9 pagesCareer Map Assignmentapi-301456362No ratings yet
- Meniere's DiseaseDocument46 pagesMeniere's Diseaseabhinay_1712No ratings yet
- Study 1 Supplementary SandplayDocument6 pagesStudy 1 Supplementary SandplayAbdullah TarekNo ratings yet
- Hazardous Materials Storage GuidelinesDocument4 pagesHazardous Materials Storage Guidelinesclinton sampsonNo ratings yet
- New DOH Hospital Classifications 2015: GovernmentDocument3 pagesNew DOH Hospital Classifications 2015: GovernmentCatherine PurisimaNo ratings yet
- Hospital MarketinDocument47 pagesHospital Marketinchandraprakash_shuklNo ratings yet
- Ultrasound Diagnosis and Management of Intra-Uterine GrowthDocument7 pagesUltrasound Diagnosis and Management of Intra-Uterine GrowthPablo VispoNo ratings yet
- HemivaginaDocument3 pagesHemivaginafitriamarizkaNo ratings yet
- Unit VI L&D Case StudyDocument6 pagesUnit VI L&D Case StudyBrooke Misty Ann BaileyNo ratings yet
- Aids Quiz: The Answer Is DDocument4 pagesAids Quiz: The Answer Is DagarhemantNo ratings yet
- Incestuous WorkplaceDocument328 pagesIncestuous WorkplacewhatamjohnbnyNo ratings yet
- Novilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Universal Precautions (UP)Document26 pagesUniversal Precautions (UP)Avigael Gabriel AvilesNo ratings yet
- What Are Foodborne Illnesses?Document5 pagesWhat Are Foodborne Illnesses?Sunday JamesNo ratings yet
- Charity Food Project Proposal Template-42293Document4 pagesCharity Food Project Proposal Template-42293Mohamed Mohideen SarhoonNo ratings yet
- MSDS 984229Document16 pagesMSDS 984229anibal_rios_rivasNo ratings yet
- Unhealthy Food Food Items Effects of Unhealthy Food ChipsDocument3 pagesUnhealthy Food Food Items Effects of Unhealthy Food ChipsM. Amebari NongsiejNo ratings yet
- EtikaDocument15 pagesEtikaWidya PratiwiNo ratings yet