You might also like
- Human Sexuality in A Changing World 10th Edition.c2Document625 pagesHuman Sexuality in A Changing World 10th Edition.c2jakeNo ratings yet
- Vaginal Birth After Caesarean (Vbac) : Max Brinsmead MB Bs PHD December 2015Document36 pagesVaginal Birth After Caesarean (Vbac) : Max Brinsmead MB Bs PHD December 2015kikyNo ratings yet
- Vbac FinDocument15 pagesVbac FinCindy AgustinNo ratings yet
- LaparotomyDocument36 pagesLaparotomydenekeNo ratings yet
- General AnesthesiaDocument27 pagesGeneral AnesthesiadenekeNo ratings yet
- 13complications of 3rd Stage of Labour MCQDocument10 pages13complications of 3rd Stage of Labour MCQKamal El-Ghorory75% (4)
- Living with Metastatic Breast Cancer: Stories of Faith and HopeFrom EverandLiving with Metastatic Breast Cancer: Stories of Faith and HopeNo ratings yet
- PQCNC OBH Kickoff CMOP Learning Session - Maternal Mortality Closing The Gap 2017Document58 pagesPQCNC OBH Kickoff CMOP Learning Session - Maternal Mortality Closing The Gap 2017kcochran100% (1)
- Lameshow Statistik PDFDocument247 pagesLameshow Statistik PDFqel_harizah100% (1)
- Postterm PregnancyDocument16 pagesPostterm PregnancyrranindyaprabasaryNo ratings yet
- 2AN Group 3 Script/Flow For RLE CHN Duty RotationDocument8 pages2AN Group 3 Script/Flow For RLE CHN Duty RotationLouwella RamosNo ratings yet
- Vbac Acog 2010Document27 pagesVbac Acog 2010ariniNo ratings yet
- Predicting Cesarean Section AnDocument5 pagesPredicting Cesarean Section AnKEANNA ZURRIAGANo ratings yet
- Managing Women With Previous CS2Document27 pagesManaging Women With Previous CS2zynal20038222No ratings yet
- IOSRPHRDocument3 pagesIOSRPHRIOSR Journal of PharmacyNo ratings yet
- Bahan Utk VCDocument58 pagesBahan Utk VCTias DiahNo ratings yet
- Vaginal Delivery of TwinsDocument63 pagesVaginal Delivery of Twinsrake sardevaNo ratings yet
- Cervical Conization and The Risk of Preterm DeliveryDocument11 pagesCervical Conization and The Risk of Preterm DeliveryGelo ConcepcionNo ratings yet
- Bang UcupDocument34 pagesBang Ucupvannyanoy100% (1)
- My Pap Smear Is Abnormal !Document70 pagesMy Pap Smear Is Abnormal !Alena JosephNo ratings yet
- Caesarean SectionDocument29 pagesCaesarean SectionMuriel CardosoNo ratings yet
- Childbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyDocument54 pagesChildbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyVeronica MendozaNo ratings yet
- Statistics BusysprDocument25 pagesStatistics BusysprKeeranmayeeishraNo ratings yet
- Vaginal Birth After Cesarean, JurnalDocument19 pagesVaginal Birth After Cesarean, Jurnaldewi trisnaNo ratings yet
- C-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Document7 pagesC-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Aris SugiatnoNo ratings yet
- 12 .Tyraskis2017Document31 pages12 .Tyraskis2017dw21541No ratings yet
- Mid-Trimester Amniocentesis Fetal Loss Rate: Committee OpinionDocument5 pagesMid-Trimester Amniocentesis Fetal Loss Rate: Committee OpinionDivine Grace ValenzuelaNo ratings yet
- Placenta PreviaDocument5 pagesPlacenta PreviaYolanda Angulo BazánNo ratings yet
- Induction of Labour Versus Expectant Management For Nulliparous Women Over 35 Years of Age: A Multi-Centre Prospective, Randomised Controlled TrialDocument8 pagesInduction of Labour Versus Expectant Management For Nulliparous Women Over 35 Years of Age: A Multi-Centre Prospective, Randomised Controlled TrialAndinNo ratings yet
- 18B# Vaginal Birth After Cesarean Section PONEK 2020Document22 pages18B# Vaginal Birth After Cesarean Section PONEK 2020ruang obstetriNo ratings yet
- In Vitro Fertilization For M6 Students: YL TsaiDocument49 pagesIn Vitro Fertilization For M6 Students: YL TsaiLee BoborasNo ratings yet
- Cesarean VsDocument8 pagesCesarean Vsapi-427591170No ratings yet
- Vbac - YurDocument20 pagesVbac - YurkikiNo ratings yet
- Vaginal Birth After Cesarean Delivery (VBAC) Definition/AbbreviationDocument3 pagesVaginal Birth After Cesarean Delivery (VBAC) Definition/AbbreviationCalvin TranNo ratings yet
- Uteri Ne Rupture Duri NG Labor Among Women With P R Ior Cesar Ean Deliver YDocument22 pagesUteri Ne Rupture Duri NG Labor Among Women With P R Ior Cesar Ean Deliver Yzero thirteen eighty oneNo ratings yet
- Prior Cesarean Delivery: 100 Years of ControversyDocument17 pagesPrior Cesarean Delivery: 100 Years of ControversyNoahYudhaNo ratings yet
- Cervical Stitch Give Birth Kelompok 2Document78 pagesCervical Stitch Give Birth Kelompok 2Larose Rossyta SariNo ratings yet
- Caesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort StudyDocument9 pagesCaesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort Studyluis albenis mendoza guerraNo ratings yet
- Cesarean DeliveryDocument13 pagesCesarean DeliveryCindy LidiaNo ratings yet
- Maternal Morbidity Associated With Multiple Repeat Cesarean DeliveriesDocument7 pagesMaternal Morbidity Associated With Multiple Repeat Cesarean Deliveriesdewi wahyuniNo ratings yet
- Critical Appraisal Ayu RonoDocument41 pagesCritical Appraisal Ayu Ronoamarendra WardhanaNo ratings yet
- Identifying Risk Factors For Uterine RuptureDocument15 pagesIdentifying Risk Factors For Uterine RuptureSakena NurzaNo ratings yet
- Knight Et Al-2014-BJOG An International Journal of Obstetrics & GynaecologyDocument10 pagesKnight Et Al-2014-BJOG An International Journal of Obstetrics & GynaecologyAndrian drsNo ratings yet
- 06 SC AlarmDocument34 pages06 SC AlarmYosie Yulanda PutraNo ratings yet
- 730 2113 1 PBDocument7 pages730 2113 1 PBFitrahMyatunNo ratings yet
- Vaginal BirthDocument7 pagesVaginal BirthMentari Cipta SeptikaNo ratings yet
- Uterine Rupture After Previous Caesarean Section: EpidemiologyDocument12 pagesUterine Rupture After Previous Caesarean Section: EpidemiologymacNo ratings yet
- Jurnal SCDocument3 pagesJurnal SCmorningNo ratings yet
- To Vbac or Not To Vbac: PerspectiveDocument3 pagesTo Vbac or Not To Vbac: Perspectiveharani roimaNo ratings yet
- Evidence Based: Vaginal Birth After Cesarean: First ResearchDocument2 pagesEvidence Based: Vaginal Birth After Cesarean: First ResearchGodfrey AntolinNo ratings yet
- Cervical Cancer Screening Recommendations, 2012: The American Society For Colposcopy and Cervical PathologyDocument55 pagesCervical Cancer Screening Recommendations, 2012: The American Society For Colposcopy and Cervical PathologyKharisma AlifahNo ratings yet
- Vbac Success 2013Document6 pagesVbac Success 2013040193izmNo ratings yet
- Pregnancy Outcome of Single Previous Cesarean SectionDocument4 pagesPregnancy Outcome of Single Previous Cesarean SectionDhesy WildayaniNo ratings yet
- Practice Bulletin: Vaginal Birth After Previous Cesarean DeliveryDocument14 pagesPractice Bulletin: Vaginal Birth After Previous Cesarean DeliveryFernando González PeruggiNo ratings yet
- 2.april 2020 Estimation of Risk Factors For MultiparousDocument4 pages2.april 2020 Estimation of Risk Factors For MultiparousTushar BahetiNo ratings yet
- Factors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaDocument8 pagesFactors Associated With Successful Vaginal Birth After Cesarean Section and Outcomes in Rural Area of AnatoliaIllona SaharaNo ratings yet
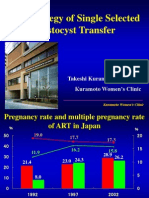
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDocument43 pagesThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiNo ratings yet
- Acta Obstet Gynecol Scand 2018 Lindblad Wollmann Risk of Repeat Cesarean Delivery in Women Undergoing Trial of LaborDocument6 pagesActa Obstet Gynecol Scand 2018 Lindblad Wollmann Risk of Repeat Cesarean Delivery in Women Undergoing Trial of LaborMillennials ShopifyNo ratings yet
- Simcox 2009Document6 pagesSimcox 2009Aulya ArchuletaNo ratings yet
- BMC Pregnancy and Childbirth: Jodie M Dodd, Caroline A Crowther, Janet E Hiller, Ross R Haslam and Jeffrey S RobinsonDocument9 pagesBMC Pregnancy and Childbirth: Jodie M Dodd, Caroline A Crowther, Janet E Hiller, Ross R Haslam and Jeffrey S RobinsonSyahrullah Ramadhan UllaNo ratings yet
- Cesarean Birth Mothering PonteDocument16 pagesCesarean Birth Mothering PonteL. BarriolaNo ratings yet
- Previous Preterm Cesarean Delivery and Risk of Uterine Rupturein Subsequent Trial of LaborDocument28 pagesPrevious Preterm Cesarean Delivery and Risk of Uterine Rupturein Subsequent Trial of LaborDjlatino LatinoNo ratings yet
- Labour Admission Test: International Journal of Infertility and Fetal Medicine December 2011Document8 pagesLabour Admission Test: International Journal of Infertility and Fetal Medicine December 2011IndhumathiNo ratings yet
- Low Primary Cesarean Rate and High VBAC Rate With Good Outcomes in An Amish Birthing CenterDocument8 pagesLow Primary Cesarean Rate and High VBAC Rate With Good Outcomes in An Amish Birthing CenterStefanichalisnia 96No ratings yet
- Twins PecepDocument8 pagesTwins Pecepjj_cani91No ratings yet
- Meaza Respiratory FinalDocument85 pagesMeaza Respiratory FinaldenekeNo ratings yet
- BurnDocument30 pagesBurndenekeNo ratings yet
- EngDocument65 pagesEngWhinet Jojo TerunaNo ratings yet
- Chest TubeDocument22 pagesChest TubedenekeNo ratings yet
- FB and CellulitisDocument42 pagesFB and CellulitisdenekeNo ratings yet
- Surgicla TechniqueDocument47 pagesSurgicla TechniquedenekeNo ratings yet
- CHAPTER 1-Intro Duction of AnesthesiaDocument28 pagesCHAPTER 1-Intro Duction of AnesthesiadenekeNo ratings yet
- Wound HealingDocument47 pagesWound HealingdenekeNo ratings yet
- Spinal AnesthesiaDocument29 pagesSpinal AnesthesiadenekeNo ratings yet
- Neonatal Resusitation NIME 2009Document55 pagesNeonatal Resusitation NIME 2009denekeNo ratings yet
- Approach To Surgical PTDocument31 pagesApproach To Surgical PTdenekeNo ratings yet
- 21.diabetes Mellitus in PregnancyDocument47 pages21.diabetes Mellitus in Pregnancydeneke100% (1)
- Preterm Labor and DeliveryDocument21 pagesPreterm Labor and DeliverydenekeNo ratings yet
- Spinal AnesthesiaDocument29 pagesSpinal AnesthesiadenekeNo ratings yet
- HypertDocument2 pagesHypertdenekeNo ratings yet
- Motor LesionsDocument30 pagesMotor Lesionsdeneke0% (1)
- 10.multiple GestationDocument49 pages10.multiple GestationdenekeNo ratings yet
- Infective Endo.Document8 pagesInfective Endo.denekeNo ratings yet
- Pyramidal TractDocument48 pagesPyramidal TractdenekeNo ratings yet
- 17 IugrDocument48 pages17 IugrdenekeNo ratings yet
- CPRDocument52 pagesCPRdenekeNo ratings yet
- 3.Dxs of PregnancyDocument24 pages3.Dxs of PregnancydenekeNo ratings yet
- 26 PcosDocument66 pages26 PcosdenekeNo ratings yet
- 5 AncDocument40 pages5 AncdenekeNo ratings yet
- 16 PromDocument18 pages16 PromdenekeNo ratings yet
- 16 PromDocument18 pages16 PromdenekeNo ratings yet
- 8.perinatal DXDocument35 pages8.perinatal DXdenekeNo ratings yet
- Guide To SexDocument16 pagesGuide To SexNiţu MarianNo ratings yet
- Essay On EmONC On Reducing Maternal MortalityDocument3 pagesEssay On EmONC On Reducing Maternal MortalityBenjaminNo ratings yet
- UNIT 5 LAB Technological Timeline Mariam SalhienDocument5 pagesUNIT 5 LAB Technological Timeline Mariam SalhienMariam SalhienNo ratings yet
- Case Scenario IDocument2 pagesCase Scenario IGynesis Lim RoqueroNo ratings yet
- Activity Sheets in Science 5 Quarter 2, Week 1: Parts of The Reproductive System and Their FunctionsDocument6 pagesActivity Sheets in Science 5 Quarter 2, Week 1: Parts of The Reproductive System and Their Functionsricardo salayonNo ratings yet
- Ectopic PregnancyDocument38 pagesEctopic PregnancyLovelyjade ReyesNo ratings yet
- The Perception of Pregnant Women Towards Antenatal Care at Madina Polyclinic-Ghana: A Descriptive Exploratory StudyDocument13 pagesThe Perception of Pregnant Women Towards Antenatal Care at Madina Polyclinic-Ghana: A Descriptive Exploratory StudyP'Babe Cece AdumoahNo ratings yet
- Save The GirlDocument11 pagesSave The GirlMeenakshi HandaNo ratings yet
- Preterm Prelabor Rupture of Membranes - Management and Outcome - UpToDateDocument35 pagesPreterm Prelabor Rupture of Membranes - Management and Outcome - UpToDatemaminyaarNo ratings yet
- Elden Ring (Video Game) - Works Archive of Our OwnDocument1 pageElden Ring (Video Game) - Works Archive of Our OwnAndrew ABell0% (1)
- PLGF Pelican Study Key PointsDocument3 pagesPLGF Pelican Study Key PointsGabriel Cadavid GilNo ratings yet
- Fetal Death in Utero Radiology Reference Article PDFDocument1 pageFetal Death in Utero Radiology Reference Article PDFMoe Wai MyintNo ratings yet
- BrochureDocument20 pagesBrochureAnjali MohanNo ratings yet
- Mechanisms of Action and Effectiveness of Contraception MethodsDocument2 pagesMechanisms of Action and Effectiveness of Contraception Methodsjaimedelafuente22No ratings yet
- Microgest InsertDocument1 pageMicrogest InsertChodhur BhodhurNo ratings yet
- Hubungan Karakteristik Ibu Inpartu Terhadap Kejadian Perdarahan Postpartum Di Rsu Budi Kemuliaan Periode Tahun 2019Document10 pagesHubungan Karakteristik Ibu Inpartu Terhadap Kejadian Perdarahan Postpartum Di Rsu Budi Kemuliaan Periode Tahun 2019MiMa Muach LadyzNo ratings yet
- High-Risk Pregnancy Premature Rupture of Membranes (PROM)Document3 pagesHigh-Risk Pregnancy Premature Rupture of Membranes (PROM)elimcangcoNo ratings yet
- CHN and OBDocument91 pagesCHN and OBJoshua Christian GanNo ratings yet
- Menstrual Cycle and Ovulation Period PDFDocument3 pagesMenstrual Cycle and Ovulation Period PDFSalman AmirNo ratings yet
- Ucsp Kinship and FamilyDocument9 pagesUcsp Kinship and FamilycdcheijdnekjdNo ratings yet
- Multiple PregnancyDocument28 pagesMultiple PregnancyFarxan Da Napolian BwoyNo ratings yet
- Obg Icd-10 Pregnancy, Childbirth, PuerperiumDocument11 pagesObg Icd-10 Pregnancy, Childbirth, PuerperiumarifianjuariNo ratings yet
- Oligohydramnios - Etiology, Diagnosis, and Management - UpToDateDocument23 pagesOligohydramnios - Etiology, Diagnosis, and Management - UpToDateJUAN FRANCISCO OSORIO PENALOZANo ratings yet
- Childhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenDocument9 pagesChildhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenScott PymNo ratings yet
- 1151 3608 1 PBDocument7 pages1151 3608 1 PBNilam SariNo ratings yet
- Nhs Forth Valley: Management of Acute Inversion of UterusDocument5 pagesNhs Forth Valley: Management of Acute Inversion of UterusMelissa Aina Mohd YusofNo ratings yet
- Dip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Document1 pageDip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Neo Latoya MadunaNo ratings yet