You might also like
- Harrison TablesDocument163 pagesHarrison Tablesfrancieudo1No ratings yet
- Hi Yield Notes in SurgeryDocument16 pagesHi Yield Notes in SurgeryNiñoTan100% (2)
- Abx FinalDocument3 pagesAbx Finalyanks1120No ratings yet
- Psychiatry MnemonicsDocument7 pagesPsychiatry MnemonicsFahad Almalki93% (15)
- Step 1 DrugsDocument19 pagesStep 1 Drugssplinter59490% (20)
- SketchyMicro ChartDocument14 pagesSketchyMicro ChartSonia100% (8)
- Free AssociationDocument10 pagesFree AssociationimorkzoneNo ratings yet
- ChartDocument5 pagesChartWesley CooperNo ratings yet
- Sexually Transmitted Disease or STI Complete SymtomsDocument11 pagesSexually Transmitted Disease or STI Complete SymtomsPowerzNo ratings yet
- Charts For Kidney and Lower Urinary Tract Pathology. NephrologyDocument34 pagesCharts For Kidney and Lower Urinary Tract Pathology. NephrologyM PatelNo ratings yet
- Hallmark Findings PDFDocument4 pagesHallmark Findings PDFGIST (Gujarat Institute of Science & Technology)No ratings yet
- Nbme 100Document11 pagesNbme 100stndNo ratings yet
- Flashcards FinalDocument272 pagesFlashcards FinalMarie SantoroNo ratings yet
- Endocrine Pathology p17-32Document16 pagesEndocrine Pathology p17-32zeroun24No ratings yet
- Differential Diagnosis of Glomerular DiseasesDocument2 pagesDifferential Diagnosis of Glomerular DiseasesMaryam Fadah100% (1)
- High Yield Goljan Path ReviewDocument57 pagesHigh Yield Goljan Path Reviewnewmexicoomfs100% (5)
- Step 1 Micro ChartsDocument38 pagesStep 1 Micro ChartsRitika AgarwalNo ratings yet
- Chapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of DiseaseDocument12 pagesChapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of DiseaseArun Nayak86% (7)
- Pharma Super TableDocument56 pagesPharma Super TableMarco Paulo Reyes NaoeNo ratings yet
- Pathology 20mnemonics 1 PDFDocument12 pagesPathology 20mnemonics 1 PDFEliza Spark100% (5)
- Pathology Description/Buzz Words DiseaseDocument5 pagesPathology Description/Buzz Words Diseasebea manzanoNo ratings yet
- Bacteria ChartsDocument11 pagesBacteria ChartsFlowerNo ratings yet
- Microbiology Table 1.23123Document8 pagesMicrobiology Table 1.23123Hanif GandohNo ratings yet
- Micro Final Buzz Word CheatsheetDocument10 pagesMicro Final Buzz Word CheatsheetThesmith FamNo ratings yet
- Sketchy Pharm Table of ContentsDocument12 pagesSketchy Pharm Table of ContentsMal G100% (1)
- Biostatistics Epidemiology Definitions ChartDocument10 pagesBiostatistics Epidemiology Definitions ChartM PatelNo ratings yet
- Anemias ChartDocument14 pagesAnemias ChartM Patel100% (2)
- Pathology NotesDocument29 pagesPathology NotesMK100% (1)
- USMLE Flashcards: Pharmacology - Side by SideDocument178 pagesUSMLE Flashcards: Pharmacology - Side by SideMedSchoolStuff67% (3)
- TOPNOTCH Patho Supplement Handout For Sept 2018 UPDATED May 2018Document25 pagesTOPNOTCH Patho Supplement Handout For Sept 2018 UPDATED May 2018Waiwit KritayakiranaNo ratings yet
- Name Types Disease Mechanism AE Other C. Cycle Resistance (CP Pg. 326) Alkylating AgentsDocument12 pagesName Types Disease Mechanism AE Other C. Cycle Resistance (CP Pg. 326) Alkylating AgentsM PatelNo ratings yet
- Sketchy Micro Table of Contents - PharmacologyDocument5 pagesSketchy Micro Table of Contents - Pharmacologymarandr100% (3)
- VirusesDocument2 pagesVirusesgregoryvo100% (4)
- Miasm AnalysisDocument6 pagesMiasm AnalysisSatyendra Rawat100% (1)
- Micro I ReviewDocument15 pagesMicro I ReviewEmilee Tu100% (1)
- ImmunologyDocument80 pagesImmunologyMaged HusseinNo ratings yet
- Microbiology - Bacteria Summary (Updated)Document26 pagesMicrobiology - Bacteria Summary (Updated)moZZeltovNo ratings yet
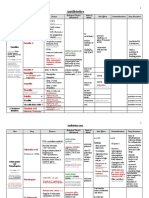
- Antibiotics ChartDocument10 pagesAntibiotics Chartadom09No ratings yet
- Infectious Disease Pathology p31-55Document25 pagesInfectious Disease Pathology p31-55zeroun2450% (2)
- Antimicrobial Drugs TableDocument19 pagesAntimicrobial Drugs TableLaylee ClareNo ratings yet
- DERM NotesDocument19 pagesDERM NoteszakyNo ratings yet
- USMLE STEP 1: Microbiology Bug List With Drugs Bugs Drugs: Bacteriology BacteriologyDocument4 pagesUSMLE STEP 1: Microbiology Bug List With Drugs Bugs Drugs: Bacteriology BacteriologymkhararahNo ratings yet
- Antibiotics Quick ReviewDocument5 pagesAntibiotics Quick Reviewpranjl100% (5)
- Mnemonics For Antibiotics-2Document10 pagesMnemonics For Antibiotics-2totallyfakeusernameNo ratings yet
- GYNE 4.02 - Lower and Upper Genital InfectionDocument12 pagesGYNE 4.02 - Lower and Upper Genital InfectionGray Snell100% (1)
- Surgery Oral ExamDocument46 pagesSurgery Oral ExamM Patel100% (9)
- Virology - Study GuideDocument5 pagesVirology - Study GuideMatt McGlothlinNo ratings yet
- MicrobesDocument12 pagesMicrobesDiMa MarshNo ratings yet
- Allure USA 2013-09Document256 pagesAllure USA 2013-09jojolilimomo67% (3)
- Step 1 Uworld PDFDocument25 pagesStep 1 Uworld PDFRegents Park Business Center100% (1)
- Pulmonary PathologyDocument6 pagesPulmonary PathologyjamesjaanNo ratings yet
- Antenatal CareDocument19 pagesAntenatal CareIshika RoyNo ratings yet
- AntibioticsDocument6 pagesAntibioticsOccamsRazor100% (1)
- IVMS Hematology-Oncology Summary Table-Notes For USMLE Step 1 Prep.Document16 pagesIVMS Hematology-Oncology Summary Table-Notes For USMLE Step 1 Prep.Marc Imhotep Cray, M.D.100% (1)
- Nephrology FormulasDocument3 pagesNephrology FormulasM Patel0% (1)
- Microbiology Step 1 Antimicrobials ChartDocument6 pagesMicrobiology Step 1 Antimicrobials ChartM Patel100% (1)
- Microbiology Step 1 Antimicrobials ChartDocument6 pagesMicrobiology Step 1 Antimicrobials ChartM Patel100% (1)
- Microbiology Quick TableDocument2 pagesMicrobiology Quick TableCoy Nuñez100% (2)
- Antibiotics ChartDocument10 pagesAntibiotics ChartTrina Si100% (6)
- A Brief Review of MiasmsDocument21 pagesA Brief Review of MiasmsMohammad AtaNo ratings yet
- TN Pharmacology in Tables PDFDocument54 pagesTN Pharmacology in Tables PDFCean ObinaNo ratings yet
- Antimicrobial AgentsDocument3 pagesAntimicrobial AgentsErnie G. Bautista II, RN, MD100% (2)
- CarcinosinDocument42 pagesCarcinosinHilery DorrianNo ratings yet
- Microbiology Step 1 Weird Exceptions and DetailDocument10 pagesMicrobiology Step 1 Weird Exceptions and DetailLucykesh100% (2)
- Pharma Katzung TablesDocument16 pagesPharma Katzung TablesPrincess Arabia-ObedozaNo ratings yet
- Patho Robbins Sumary Pereira MDDocument22 pagesPatho Robbins Sumary Pereira MDNicole SarcosNo ratings yet
- Penicillins Pen&G Pen&V: T.%pallidum% (Syphilis)Document1 pagePenicillins Pen&G Pen&V: T.%pallidum% (Syphilis)gregoryvo100% (5)
- Oral Manifestaions of Systemic DiseasesDocument116 pagesOral Manifestaions of Systemic DiseaseslikhithaNo ratings yet
- Major Pharm ReviewDocument14 pagesMajor Pharm Reviewsarahpierre10100% (3)
- Sexually Transmitted DiseasesDocument54 pagesSexually Transmitted DiseasesMowlidAbdirahman Ali madaaleNo ratings yet
- Antifungal Agents: EchinocandinsDocument2 pagesAntifungal Agents: EchinocandinsCourtney TownsendNo ratings yet
- Staphylococcus 1Document8 pagesStaphylococcus 1JohnWangerNo ratings yet
- ClostridiumDocument44 pagesClostridiummajoragarwal1195No ratings yet
- Chapter 15 StreptococciDocument8 pagesChapter 15 Streptococcinonie jacobNo ratings yet
- Respiratory Tract MicrobiologyDocument68 pagesRespiratory Tract Microbiologysultan khabeebNo ratings yet
- Staphylococcus & StreptococcusDocument100 pagesStaphylococcus & StreptococcusFahim NadvyNo ratings yet
- Bact Fung InfectionsDocument12 pagesBact Fung InfectionsSyamil AzharNo ratings yet
- StaphylococciDocument73 pagesStaphylococcishahbaz100% (5)
- Streptococcus (Coccus Gram Positif)Document45 pagesStreptococcus (Coccus Gram Positif)arisita firmanNo ratings yet
- Tumor Genes Growth FactorsDocument4 pagesTumor Genes Growth FactorsM PatelNo ratings yet
- Cardiology Arteritis ChartDocument3 pagesCardiology Arteritis ChartM PatelNo ratings yet
- Iv. Concentric Hypertrophy: A. Increase Vent Mass Relative To VolumeDocument8 pagesIv. Concentric Hypertrophy: A. Increase Vent Mass Relative To VolumeM PatelNo ratings yet
- Psych Drugs List - To Be Filled inDocument3 pagesPsych Drugs List - To Be Filled inM Patel100% (1)
- Obstetrics Gynecology TableDocument22 pagesObstetrics Gynecology TableM PatelNo ratings yet
- Mnemonics CondensedDocument4 pagesMnemonics CondensedM PatelNo ratings yet
- BActe Chap 14Document6 pagesBActe Chap 14barbiegahibNo ratings yet
- Sexually Transmitted Diseases: Nelia B. Perez RN, MSN Class 2015Document94 pagesSexually Transmitted Diseases: Nelia B. Perez RN, MSN Class 2015Mariana CreciunNo ratings yet
- Case 25-2016: A 33-Year-Old Man With Rectal Pain and BleedingDocument7 pagesCase 25-2016: A 33-Year-Old Man With Rectal Pain and BleedingNaomi HalmNo ratings yet
- Group 2Document53 pagesGroup 2Cms CSUNo ratings yet
- MICRO Master ListDocument63 pagesMICRO Master ListDaniel Del RiscoNo ratings yet
- Block 1 (40) Infectious Diseases As-CompressedDocument173 pagesBlock 1 (40) Infectious Diseases As-CompressedanweridrisejazNo ratings yet
- Skin LMRP 2019Document21 pagesSkin LMRP 2019skNo ratings yet
- Scientific SessionDocument3 pagesScientific SessionAshpavi ArunNo ratings yet
- Diabetes Mellitus 1Document96 pagesDiabetes Mellitus 1AkeroNo ratings yet
- Historia Del Tratamiento de La Sífilis - SCIELO PDFDocument14 pagesHistoria Del Tratamiento de La Sífilis - SCIELO PDFBrenda MoralesNo ratings yet
- Centers For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesDocument6 pagesCenters For Disease Control and Prevention's Sexually Transmitted Diseases Infection GuidelinesabhinavrautNo ratings yet
- Nursing Care of The Community: Control of Communicable Diseases Instructional SlidesDocument46 pagesNursing Care of The Community: Control of Communicable Diseases Instructional SlidesJullienne Ysabelle AngNo ratings yet
- Global Progress Report On HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021Document108 pagesGlobal Progress Report On HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021Tugasbu CicikNo ratings yet
- The Tuskegee Syphilis StudyDocument11 pagesThe Tuskegee Syphilis Studyapi-285171544No ratings yet
- Antibiotic GuidelinesDocument38 pagesAntibiotic GuidelinesKomang Adhi AmertajayaNo ratings yet
- NeurosyphilisDocument2 pagesNeurosyphiliserfNo ratings yet
- SyphilisDocument25 pagesSyphilisgopscharanNo ratings yet
- Musculoskeltal ProbsDocument40 pagesMusculoskeltal ProbsmilayosoresNo ratings yet
- Reproductive Tract InfectionsDocument46 pagesReproductive Tract Infectionskb100% (1)