You might also like
- HeadgearDocument62 pagesHeadgearAmanda Rosy RoneyNo ratings yet
- PDFDocument408 pagesPDFKristelle MalicdemNo ratings yet
- Laryngeal MassageDocument6 pagesLaryngeal Massageamal100% (1)
- Module 5. NEOPLASIADocument19 pagesModule 5. NEOPLASIAKryss Renato Engel BartolomeNo ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- Surgical Pathology - CNSDocument2 pagesSurgical Pathology - CNSIsabel CastilloNo ratings yet
- Ganglioneuroma: O Adam, ES Boia, Rodica Ilie, Ramona MandruscaDocument4 pagesGanglioneuroma: O Adam, ES Boia, Rodica Ilie, Ramona MandruscaRaluca BolboaseNo ratings yet
- Osteosarcoma PDFDocument3 pagesOsteosarcoma PDFkc andrea torresNo ratings yet
- UntitledDocument2 pagesUntitledVin TagenNo ratings yet
- Additional Notes in Pedia Neuro2Document4 pagesAdditional Notes in Pedia Neuro2Geraldine Marie SalvoNo ratings yet
- AAD BF Head and Neck Lesions InfantDocument2 pagesAAD BF Head and Neck Lesions Infantkahkashanahmed065No ratings yet
- 1073 FullDocument7 pages1073 FullMaria Esther GomezNo ratings yet
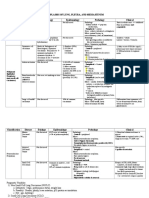
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
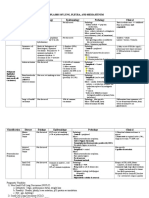
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Factor Normal Cancer CytoplasmDocument2 pagesFactor Normal Cancer CytoplasmYuji TanakaNo ratings yet
- Topic 1Document32 pagesTopic 1Exo SaranghajaNo ratings yet
- Malignant Renal Tumors 1Document2 pagesMalignant Renal Tumors 1iqz saniomeNo ratings yet
- Neoplasms of Infancy and ChildhoodDocument25 pagesNeoplasms of Infancy and ChildhoodPakeezaNo ratings yet
- Prelim GeneticsDocument3 pagesPrelim Genetics1234No ratings yet
- Oral Pathology Dent1411Document7 pagesOral Pathology Dent1411api-663458841No ratings yet
- Cancer Epidemiology Pathogenesis Lab/Gross Clinical Features Prognosis/TxDocument7 pagesCancer Epidemiology Pathogenesis Lab/Gross Clinical Features Prognosis/TxCaryn RobertsonNo ratings yet
- 5 4b Childhood Malignancy Part 2 DR Melanie Victoria G DarDocument7 pages5 4b Childhood Malignancy Part 2 DR Melanie Victoria G DarSamatha SamathaNo ratings yet
- CancerDocument18 pagesCanceralexngNo ratings yet
- Uw - Elseby Notes PediatricsDocument218 pagesUw - Elseby Notes PediatricsIvy QueenNo ratings yet
- Pathology of Neoplasia Cancer Malignant Benign Carcinoma Lecture PDFDocument8 pagesPathology of Neoplasia Cancer Malignant Benign Carcinoma Lecture PDFjax111No ratings yet
- Bladder Tumors: Normal AnatomyDocument11 pagesBladder Tumors: Normal AnatomyPankaj DubeyNo ratings yet
- Overview Neoplasia FKG PDFDocument8 pagesOverview Neoplasia FKG PDFrona angelin purbaNo ratings yet
- TumorDocument5 pagesTumori gede ricky jaya purnawarmanNo ratings yet
- Jadp 09 321Document8 pagesJadp 09 321Diornald MogiNo ratings yet
- Childhood TumorsDocument1 pageChildhood TumorsChege AmbroseNo ratings yet
- Pathology Week8 NeoplasiaDocument13 pagesPathology Week8 NeoplasiaSalifyanji SimpambaNo ratings yet
- Breast Cancer (Aka BR CA) : - Routine Screening For Genetic Abnormalities of A Strong Family HX of BR CA Is NOT NeededDocument6 pagesBreast Cancer (Aka BR CA) : - Routine Screening For Genetic Abnormalities of A Strong Family HX of BR CA Is NOT NeededChanthorn SokNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- Update On Childhood Rhabdomyosarcoma: ReviewDocument4 pagesUpdate On Childhood Rhabdomyosarcoma: ReviewPhn StanleyNo ratings yet
- 409 FullDocument11 pages409 FullMario QuinteroNo ratings yet
- Overview Diagnosis and Treatment of GI NETSDocument73 pagesOverview Diagnosis and Treatment of GI NETSΒΑΣΙΛΗΣ ΚΟΛΙΝΤΖΙΚΗΣNo ratings yet
- Patho DermatologyDocument16 pagesPatho DermatologyChristian CastueraNo ratings yet
- Esophagus TumorsDocument5 pagesEsophagus TumorsblablalbablablablaNo ratings yet
- Rangkuman TumorDocument31 pagesRangkuman TumorraishapiNo ratings yet
- Atypical Spitz Tumors: A Diagnostic ChallengeDocument8 pagesAtypical Spitz Tumors: A Diagnostic ChallengeCristi PopescuNo ratings yet
- GCT Giant Cell Tumor PresentationDocument22 pagesGCT Giant Cell Tumor PresentationHasyasya Furnita KosaziNo ratings yet
- Chapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFDocument9 pagesChapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFChethranNo ratings yet
- Path Adrenal TumorDocument4 pagesPath Adrenal TumorRama HijaziNo ratings yet
- Theoncologist 2016-0079Document12 pagesTheoncologist 2016-0079IlincaNo ratings yet
- 1 s2.0 S1319453412001075 MainDocument11 pages1 s2.0 S1319453412001075 Maincdcruzb1996No ratings yet
- CancerDocument17 pagesCancerShyenNo ratings yet
- SynoviomaDocument28 pagesSynoviomaAnonymous bE4VegCcNo ratings yet
- Neurology NotesDocument1 pageNeurology NotesTharaniNo ratings yet
- Genetic News: Impact Chromosomal Aberrations Can Have On A Variety of Syndromes By: Alessandra BassaniDocument4 pagesGenetic News: Impact Chromosomal Aberrations Can Have On A Variety of Syndromes By: Alessandra Bassaniapi-308289644No ratings yet
- College of Dentistry - General Pathology: Course Material: NeoplasiaDocument66 pagesCollege of Dentistry - General Pathology: Course Material: NeoplasiaVincent De AsisNo ratings yet
- Curr Diag Pathol-2006-12 - Sinonasal CarcinomasDocument14 pagesCurr Diag Pathol-2006-12 - Sinonasal Carcinomasdarmayanti ibnuNo ratings yet
- Tumors of The Orbit by Dr. Jonathan Del Prado 082708Document3 pagesTumors of The Orbit by Dr. Jonathan Del Prado 082708CitrusNo ratings yet
- Shafiq Sir All GFBDocument110 pagesShafiq Sir All GFBAbir WahidNo ratings yet
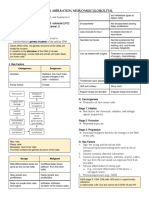
- Eca - Cellular Aberration-Neuro-MusculoskeletalDocument29 pagesEca - Cellular Aberration-Neuro-MusculoskeletalFrancis Alfred EscaranNo ratings yet
- Noonan Syndrome (Am Fam Physician. 2014 PDFDocument7 pagesNoonan Syndrome (Am Fam Physician. 2014 PDFKhalila DiantiNo ratings yet
- Musculoskeletal ChartsDocument27 pagesMusculoskeletal Chartssurviving nursing school100% (3)
- 6.4 Issues of Cell Division On Human HealthDocument23 pages6.4 Issues of Cell Division On Human Healthwickedbiology101No ratings yet
- Genetics FinalsDocument27 pagesGenetics FinalsEDLENE JOY ALBANIELNo ratings yet
- Notes DermaDocument17 pagesNotes DermaCiullaeNo ratings yet
- Finals ReviewerDocument35 pagesFinals Reviewerimlookingforyou.03No ratings yet
- Polyps AdvancedDocument5 pagesPolyps AdvancedblablalbablablablaNo ratings yet
- NeoplasiaDocument21 pagesNeoplasiaFreakyRustlee LeoragNo ratings yet
- Spun Candy Investor PresentationDocument32 pagesSpun Candy Investor PresentationMrSomnambululNo ratings yet
- Enrolment Overview: 1. Select My Student Center' From Your Myglasgow HomepageDocument16 pagesEnrolment Overview: 1. Select My Student Center' From Your Myglasgow HomepageMrSomnambululNo ratings yet
- ChitosanDocument52 pagesChitosanMrSomnambululNo ratings yet
- Chitosan: Kimberly Novak, Melanie Johns Cupp, and Timothy S. TracyDocument9 pagesChitosan: Kimberly Novak, Melanie Johns Cupp, and Timothy S. TracyMrSomnambululNo ratings yet
- 100-2010 Zhabg PDFDocument8 pages100-2010 Zhabg PDFMrSomnambululNo ratings yet
- Applications of Chitin and Chitosan in Industry and Medical Science: A ReviewDocument6 pagesApplications of Chitin and Chitosan in Industry and Medical Science: A ReviewMrSomnambululNo ratings yet
- Chapter 9 Subtract Ive MixingDocument19 pagesChapter 9 Subtract Ive MixingMrSomnambululNo ratings yet
- Chapter 9: Color Additive Primary ColorsDocument19 pagesChapter 9: Color Additive Primary ColorsMrSomnambululNo ratings yet
- Notes On HomeworkDocument19 pagesNotes On HomeworkMrSomnambululNo ratings yet
- Course Info: Dr. Ellen KeisterDocument14 pagesCourse Info: Dr. Ellen KeisterMrSomnambululNo ratings yet
- Chapter 7 Receptive Fields 2Document18 pagesChapter 7 Receptive Fields 2MrSomnambululNo ratings yet
- Chapter 4: Cameras and Photography: - Depth of Field - ExposureDocument21 pagesChapter 4: Cameras and Photography: - Depth of Field - ExposureMrSomnambululNo ratings yet
- Chapter 5 EyeDocument14 pagesChapter 5 EyeMrSomnambululNo ratings yet
- Homework Policies: - Molly: Tuesdays 2-4pm - Dr. Keister: Wednesdays 10am-12 - Prof. Goldman: Wednesdays 2-3:30pmDocument14 pagesHomework Policies: - Molly: Tuesdays 2-4pm - Dr. Keister: Wednesdays 10am-12 - Prof. Goldman: Wednesdays 2-3:30pmMrSomnambululNo ratings yet
- 12taste and SmellDocument19 pages12taste and SmellMrSomnambululNo ratings yet
- L 10 BalanceDocument11 pagesL 10 BalanceMrSomnambululNo ratings yet
- The Physiology of The Senses - Touch, Pain, Taste and SmellDocument20 pagesThe Physiology of The Senses - Touch, Pain, Taste and SmellMrSomnambululNo ratings yet
- List Obat Baru Dan Obat Kosong DistributorDocument16 pagesList Obat Baru Dan Obat Kosong DistributorDamay KartikaNo ratings yet
- Essential Drugs For Subclinic UseDocument9 pagesEssential Drugs For Subclinic UseGebremichael RetaNo ratings yet
- CRT Exam Review Guide Chapter 8Document10 pagesCRT Exam Review Guide Chapter 8Dharlyn MungcalNo ratings yet
- List of Instruments For Part II ExaminationDocument32 pagesList of Instruments For Part II ExaminationananthNo ratings yet
- Nicole M. Hendrickson: ProfessionDocument2 pagesNicole M. Hendrickson: ProfessionDavidNo ratings yet
- Hepatobiliary Case StudyDocument7 pagesHepatobiliary Case Studyapi-329630557No ratings yet
- Drug Study Blank SheetDocument2 pagesDrug Study Blank SheetAfia TawiahNo ratings yet
- Decision Making in Veterinary Practice Barry Kipperman Full ChapterDocument67 pagesDecision Making in Veterinary Practice Barry Kipperman Full Chaptermelvin.white671100% (3)
- APPENDIX B-Comparative HematologyDocument30 pagesAPPENDIX B-Comparative HematologySultan AlexandruNo ratings yet
- Hepatitis Role Ayurveda Article BhaktiDocument12 pagesHepatitis Role Ayurveda Article BhaktiDr. Bhakti PatilNo ratings yet
- Cancer Mother of All Diseases ASU Study Guide Exam #1Document2 pagesCancer Mother of All Diseases ASU Study Guide Exam #1Nitin NandaNo ratings yet
- 01d MCQ and A Intro To Man Acc and Cost ConceptsDocument8 pages01d MCQ and A Intro To Man Acc and Cost ConceptsK Lam LamNo ratings yet
- Development and Characterization of Transdermal Patch For Controlled Release of Fluocinolone AcetonideDocument12 pagesDevelopment and Characterization of Transdermal Patch For Controlled Release of Fluocinolone AcetonideJOURNAL CLUB FOR PHARMACEUTICAL SCIENCES (JCPS)No ratings yet
- 1e PICOT Questions TemplateDocument2 pages1e PICOT Questions TemplateZvonka FekonjaNo ratings yet
- Classical and Operant Conditioning: Group 1 Shravan Abraham Ashwini Sindura Sadanandan Sneha JohnDocument15 pagesClassical and Operant Conditioning: Group 1 Shravan Abraham Ashwini Sindura Sadanandan Sneha JohnSindura SadanandanNo ratings yet
- Module 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionDocument229 pagesModule 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionA.h.MuradNo ratings yet
- Jurnal Dyan SamsaraDocument18 pagesJurnal Dyan SamsaraDaily Alman&momNo ratings yet
- Fundamental Nursing PracticeDocument23 pagesFundamental Nursing PracticeChristine MagbataNo ratings yet
- Hps Health - Indian Sanskrit Damar Tantra Sutra (Part 5), Urine TherapyDocument4 pagesHps Health - Indian Sanskrit Damar Tantra Sutra (Part 5), Urine TherapyAashishh PatilNo ratings yet
- VVStages of Behaviour, Fagerstorm Score and CO AnalyzerDocument45 pagesVVStages of Behaviour, Fagerstorm Score and CO AnalyzerUnit NCD PKDSPUNo ratings yet
- CTH SBA Sample Questions FINALDocument1 pageCTH SBA Sample Questions FINALMD Luthfy LubisNo ratings yet
- Notch DependenceDocument29 pagesNotch DependencepnavasterNo ratings yet
- SurabhiDocument11 pagesSurabhickbhaiNo ratings yet
- Samarpan BiologyDocument23 pagesSamarpan Biologyblack kobraNo ratings yet
- Brief Psychiatric Rating ScaleDocument1 pageBrief Psychiatric Rating ScalesilmarestuNo ratings yet
- Seminar Report by Shashank AroraDocument33 pagesSeminar Report by Shashank AroraSanjay JangidNo ratings yet
- 500 Item Free Nursing Board Exam ReviewerDocument149 pages500 Item Free Nursing Board Exam ReviewerMichael Montaño100% (3)