You might also like
- Lieutenant Commander Anthony DiNozzo Pt.1Document23 pagesLieutenant Commander Anthony DiNozzo Pt.1hurricanesea81% (21)
- NCLEX-RN Q&A Flash Cards by Ray A. Hargrove-Huttel, Kathryn Cadenhead ColgroDocument793 pagesNCLEX-RN Q&A Flash Cards by Ray A. Hargrove-Huttel, Kathryn Cadenhead ColgroHeri Zalmes Dodge Tomahawk94% (53)
- 82-P01.91.300393-04 KT-60 Operation ManualDocument158 pages82-P01.91.300393-04 KT-60 Operation ManualWolaé Mathurin Edmond AmegandjinNo ratings yet
- Guyton Chapter 36Document6 pagesGuyton Chapter 36g_komolafe100% (1)
- The Song of The ButterfliesDocument345 pagesThe Song of The ButterfliesNicole Anne PerezNo ratings yet
- Case Study 04 Ford PintoDocument12 pagesCase Study 04 Ford PintoFlorentina CocoşNo ratings yet
- Haemostasis: DR Sri Lestari Sulistyo Rini, MSCDocument56 pagesHaemostasis: DR Sri Lestari Sulistyo Rini, MSCelfianaNo ratings yet
- Normal HemostasisDocument34 pagesNormal Hemostasisمصطفي خندقاويNo ratings yet
- Hemostasis: Presenter-Dr. SonuDocument68 pagesHemostasis: Presenter-Dr. SonukiranNo ratings yet
- 11-Components of The Haemostatic ResponseDocument45 pages11-Components of The Haemostatic ResponseNipun ShamikaNo ratings yet
- Haematology Lecture 7+8Document34 pagesHaematology Lecture 7+8Nabeel TahirNo ratings yet
- Components of The HaemostaticDocument25 pagesComponents of The HaemostaticRo RyNo ratings yet
- Lecture 4-HemostasisDocument34 pagesLecture 4-HemostasissamayaNo ratings yet
- Hemostasis and Blood CoagulationDocument35 pagesHemostasis and Blood CoagulationHarun MohamedNo ratings yet
- Haemostasis: Case StudyDocument19 pagesHaemostasis: Case StudyTusabe FredNo ratings yet
- Platelets. Hemostasis.: Learning ObjectivesDocument37 pagesPlatelets. Hemostasis.: Learning ObjectivesQasim alaliNo ratings yet
- Haemostasis: Dr. Ali ElhassanDocument45 pagesHaemostasis: Dr. Ali ElhassanMohja JaberNo ratings yet
- 1 Blood HemostasisDocument32 pages1 Blood Hemostasisarlinda noviana100% (1)
- Bleeding DisordersDocument103 pagesBleeding Disordersabotreka056No ratings yet
- Blood Coagulation: Presenter: DR Pashi V Moderator: DR Zulu RDocument53 pagesBlood Coagulation: Presenter: DR Pashi V Moderator: DR Zulu RRabia AhmadNo ratings yet
- Seminar 4th WeekDocument33 pagesSeminar 4th WeekBibo BobiNo ratings yet
- Aula Af 2 PDFDocument49 pagesAula Af 2 PDFtobiasmanuel179No ratings yet
- Introduction To HemostasisDocument45 pagesIntroduction To Hemostasismedino100% (3)
- Hemostasis: Overview of Normal Hemostasis 3Document23 pagesHemostasis: Overview of Normal Hemostasis 3Joce Maripangui100% (1)
- Learning ObjectivesDocument12 pagesLearning ObjectivesjmcvicenteNo ratings yet
- He Most As IsDocument22 pagesHe Most As IsFiras Nazih Bou DiabNo ratings yet
- Anticoagulants, Fibrinolytics, AntiplateletsDocument88 pagesAnticoagulants, Fibrinolytics, Antiplateletspmuawiyah25No ratings yet
- Hemostasis ReviewerDocument14 pagesHemostasis ReviewerDayledaniel SorvetoNo ratings yet
- Physiology of CoagulationDocument16 pagesPhysiology of CoagulationIlyas HalimNo ratings yet
- PlateletsDocument11 pagesPlateletsislamicmedia188No ratings yet
- Platelets (Or) Thrombocytes BY U.Sivakumar: 1 PhysiologyDocument40 pagesPlatelets (Or) Thrombocytes BY U.Sivakumar: 1 PhysiologyAkash JaatNo ratings yet
- Arterial Thrombosis and EmbolismDocument43 pagesArterial Thrombosis and EmbolismA A D H INo ratings yet
- Lecture On Hemostasis by Dr. RoomiDocument43 pagesLecture On Hemostasis by Dr. RoomiMudassar Roomi100% (1)
- Coagulation CascadeDocument41 pagesCoagulation CascadeJae TNo ratings yet
- Farmakoterapi Coagulation DisorderDocument55 pagesFarmakoterapi Coagulation DisorderNur Astuty PurnamasariNo ratings yet
- Approach To Bleeding NeonateDocument20 pagesApproach To Bleeding NeonateIndranil DuttaNo ratings yet
- Introduction To HaemostasisDocument18 pagesIntroduction To Haemostasiswatchme3No ratings yet
- Blood Coagulation SeminarDocument115 pagesBlood Coagulation SeminarmeghaNo ratings yet
- Module 1 - Blood Vasculature, Megakaryocytes and PlateletsDocument31 pagesModule 1 - Blood Vasculature, Megakaryocytes and PlateletsI love dem Coffee (Migz)No ratings yet
- Hematology 5Document305 pagesHematology 5Confidence MorganNo ratings yet
- Blood Coagulation-1Document41 pagesBlood Coagulation-1samyogadkNo ratings yet
- Lecture 6 - BloodDocument5 pagesLecture 6 - Bloodadnan yaqoobNo ratings yet
- Blood Cells and CoagulationDocument26 pagesBlood Cells and CoagulationHoàngBảoLongNo ratings yet
- Schemi 1-2Document7 pagesSchemi 1-2lucaNo ratings yet
- DR Madzlifah AhadonDocument98 pagesDR Madzlifah AhadonFrances Lau Yee ChinNo ratings yet
- Chapter 35 Part 1Document31 pagesChapter 35 Part 1Gordon JamesonNo ratings yet
- ClottingDocument25 pagesClottingAtalabi AdebusolaNo ratings yet
- مستند PDF-3C57C64C1675-1Document15 pagesمستند PDF-3C57C64C1675-1lorenoh21No ratings yet
- Haemostasis: DR Stephanie LeeDocument33 pagesHaemostasis: DR Stephanie LeeOsman MNo ratings yet
- 1-2 Hemostasis PhysiologyDocument48 pages1-2 Hemostasis PhysiologyHussein Al Saedi100% (2)
- Chapter 1 Overview of IsDocument35 pagesChapter 1 Overview of IsNathalie PortugalNo ratings yet
- 11 Coagulation PDFDocument51 pages11 Coagulation PDFمحمد علي حريج / مسائيNo ratings yet
- Hema Lesson10 CoagulationDocument102 pagesHema Lesson10 CoagulationAshley RayNo ratings yet
- Bleeding TendancyDocument131 pagesBleeding TendancysamaNo ratings yet
- Bleeding Disorders1Document81 pagesBleeding Disorders1DrMuskan AroraNo ratings yet
- Bleeding Clotting Disorders I FREEMAN 20131Document90 pagesBleeding Clotting Disorders I FREEMAN 20131Elleason Joshua G. FranciscoNo ratings yet
- HemostasisDocument2 pagesHemostasisdea syafiraNo ratings yet
- HEMOSTASIS Aytona PDFDocument27 pagesHEMOSTASIS Aytona PDFMae AnnNo ratings yet
- Haemostasis Foundation 1-October 2010Document51 pagesHaemostasis Foundation 1-October 2010cute_sakura_03No ratings yet
- Platelets-Composition, Function, Hemostasis and Its Individual PhasesDocument14 pagesPlatelets-Composition, Function, Hemostasis and Its Individual PhasesHebsiba PonnayyanNo ratings yet
- Bleeding Disorders 1Document152 pagesBleeding Disorders 1Shameena KnNo ratings yet
- Hematology PPT 2Document129 pagesHematology PPT 2Saidu BobbojiNo ratings yet
- Platelet Protocols: Research and Clinical Laboratory ProceduresFrom EverandPlatelet Protocols: Research and Clinical Laboratory ProceduresNo ratings yet
- (Final1) Evidance Based GuidelinesDocument12 pages(Final1) Evidance Based Guidelinesdona donneNo ratings yet
- 17 Heart Failure DrugsDocument18 pages17 Heart Failure Drugsdona donneNo ratings yet
- 8 Supac PDFDocument18 pages8 Supac PDFdona donneNo ratings yet
- 2nd Group of Hands OutDocument15 pages2nd Group of Hands Outdona donneNo ratings yet
- 1) ECHO Model 2) Pharmacoeconomic Basic Definition and Some Notes 3) Local View 4) Basic MethodsDocument5 pages1) ECHO Model 2) Pharmacoeconomic Basic Definition and Some Notes 3) Local View 4) Basic Methodsdona donneNo ratings yet
- 6 - CardiovascularDocument22 pages6 - Cardiovasculardona donneNo ratings yet
- 2 14 2 PDFDocument3 pages2 14 2 PDFdona donneNo ratings yet
- Exam Micro 2017Document5 pagesExam Micro 2017dona donne100% (1)
- 1 IntroductionDocument68 pages1 Introductiondona donneNo ratings yet
- Eclampsia and Hellp SyndromeDocument22 pagesEclampsia and Hellp SyndromeDr-Fouad ElmaadawyNo ratings yet
- Reviewer For Skeletal SystemDocument7 pagesReviewer For Skeletal SystemRegNo ratings yet
- Brush CuttersDocument8 pagesBrush CuttersSooraj Kannan, P.V.No ratings yet
- NHL0069932 PDFDocument11 pagesNHL0069932 PDFCTV NewsNo ratings yet
- Trauma SSPDocument79 pagesTrauma SSPbbc_dkkNo ratings yet
- Ergonomic Workplace Evaluation ofDocument20 pagesErgonomic Workplace Evaluation ofFitiwi GnigusNo ratings yet
- LumbotomyDocument25 pagesLumbotomyB2PNo ratings yet
- Unit f361 Vocabulary List Excel VersionDocument25 pagesUnit f361 Vocabulary List Excel VersionbruindogNo ratings yet
- Anatomy MnemonicsDocument39 pagesAnatomy Mnemonicslynk7870% (1)
- Kenmore 385.11703 Sewing Machine Instruction ManualDocument41 pagesKenmore 385.11703 Sewing Machine Instruction ManualiliiexpugnansNo ratings yet
- Boxing ManualDocument21 pagesBoxing ManualAnonymous he11ErNo ratings yet
- Degradation of MaterialsDocument29 pagesDegradation of MaterialsjamesNo ratings yet
- Glasgow Coma ScaleDocument2 pagesGlasgow Coma ScaleAlas CuatroNo ratings yet
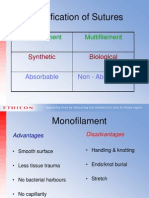
- Classification of Sutures: Monofilament MultifilamentDocument17 pagesClassification of Sutures: Monofilament Multifilamentlina_m354No ratings yet
- John Green - Looking For Alaska QuotesDocument14 pagesJohn Green - Looking For Alaska QuoteslkNo ratings yet
- What Is Physical EducationDocument35 pagesWhat Is Physical EducationAllyssa LausNo ratings yet
- 999-998-676.10 - 918-I Manual REV D 223 - Multi-4 WebDocument96 pages999-998-676.10 - 918-I Manual REV D 223 - Multi-4 WebLeonel MoralesNo ratings yet
- National Consensus Policy On Use of ForceDocument5 pagesNational Consensus Policy On Use of ForceKOLD News 13No ratings yet
- Amnesia With Focus On Post Traumatic AmnesiaDocument27 pagesAmnesia With Focus On Post Traumatic AmnesiaWilliam ClemmonsNo ratings yet
- WWI Medicine Knowledge Organiser Gcse EdexcelDocument2 pagesWWI Medicine Knowledge Organiser Gcse Edexcelrockie xoxoNo ratings yet
- Developmental Dysplasia of The HipDocument16 pagesDevelopmental Dysplasia of The Hipjonathan_alvaNo ratings yet
- SOLAS and Marine AccidentsDocument25 pagesSOLAS and Marine AccidentsAmineMeb100% (1)
- The Development of Tibiofemoral Angle in Children - Salenius e VankkaDocument3 pagesThe Development of Tibiofemoral Angle in Children - Salenius e VankkaVictor SechinNo ratings yet
- Orthopedic Chanting: by Dr. ParasDocument15 pagesOrthopedic Chanting: by Dr. ParasSaravanan DevarajNo ratings yet
- 3E Birthright - FeatsDocument10 pages3E Birthright - Featstanelorn266100% (2)