You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EASA Exam - Module 04 ElectronicsDocument115 pagesEASA Exam - Module 04 Electronicsbika100% (1)
- 1677 5538 Ibju 42 06 1220 PDFDocument8 pages1677 5538 Ibju 42 06 1220 PDFhendraNo ratings yet
- A Hydatidiform Mole Can Cause Severe Gestational HyperthyroidismDocument3 pagesA Hydatidiform Mole Can Cause Severe Gestational HyperthyroidismhendraNo ratings yet
- Mole,: Hydatidiform OccurringDocument1 pageMole,: Hydatidiform OccurringhendraNo ratings yet
- BBBBBBDocument7 pagesBBBBBBhendraNo ratings yet
- Gabapentin and Post StrokerDocument8 pagesGabapentin and Post StrokerhendraNo ratings yet
- Clinical and Radiological Correlations in Patients With Gestational Trophoblastic DiseaseDocument10 pagesClinical and Radiological Correlations in Patients With Gestational Trophoblastic DiseasehendraNo ratings yet
- Jir 7 133Document6 pagesJir 7 133hendraNo ratings yet
- Eye Surgery in The Elderly: Clinical Interventions in Aging DoveDocument8 pagesEye Surgery in The Elderly: Clinical Interventions in Aging DovehendraNo ratings yet
- Molecules 21 00143Document12 pagesMolecules 21 00143hendraNo ratings yet
- Detecting Visual Function Abnormality With A Contrast-Dependent Visual Test in Patients With Type 2 DiabetesDocument19 pagesDetecting Visual Function Abnormality With A Contrast-Dependent Visual Test in Patients With Type 2 DiabeteshendraNo ratings yet
- A Wet Dressing For Male Genital Surgery: A Phase II Clinical TrialDocument8 pagesA Wet Dressing For Male Genital Surgery: A Phase II Clinical TrialhendraNo ratings yet
- Generator Breaker Equipped With Vacuum InterruptersDocument4 pagesGenerator Breaker Equipped With Vacuum InterruptersVenna Karthik ReddyNo ratings yet
- DexX A Double Layer Unpacking Framework For AndroidDocument10 pagesDexX A Double Layer Unpacking Framework For Androidali saaedNo ratings yet
- Decision Area/s (Barangay) Hazards/Problems Technical Findings Impacts/Implications Policy InterventionsDocument2 pagesDecision Area/s (Barangay) Hazards/Problems Technical Findings Impacts/Implications Policy InterventionsCHICKYNo ratings yet
- Chapters 1, 2 & 6Document95 pagesChapters 1, 2 & 6Mwizukanji NakambaNo ratings yet
- Grade 5 Science Most Essential Learning Competencies MELCsDocument5 pagesGrade 5 Science Most Essential Learning Competencies MELCsPaul Fausto MaghirangNo ratings yet
- Sample Course Overview - TemplateDocument2 pagesSample Course Overview - TemplateSingam SridharNo ratings yet
- DOT Hazmat Training For Nuclear Medicine Technologists - Rules of The RoadDocument50 pagesDOT Hazmat Training For Nuclear Medicine Technologists - Rules of The RoadAdji Achmad J BramantyaNo ratings yet
- Busy Moms WorkoutDocument26 pagesBusy Moms WorkoutSean Licciardi100% (1)
- Lesson 1 Definition Characteristics and Branches of PhilosophyDocument55 pagesLesson 1 Definition Characteristics and Branches of PhilosophyJhasmin GierranNo ratings yet
- Call For Papers-International Journal of Wireless & Mobile Networks (IJWMN)Document2 pagesCall For Papers-International Journal of Wireless & Mobile Networks (IJWMN)John BergNo ratings yet
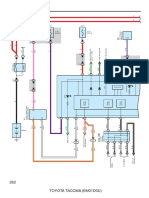
- Combination Meter: 262 Toyota Tacoma (Em01D0U)Document6 pagesCombination Meter: 262 Toyota Tacoma (Em01D0U)hamayunNo ratings yet
- PMLS 2 Midterm 1Document14 pagesPMLS 2 Midterm 1ematias230000001830No ratings yet
- B2B Project Proposal It Sector: Group 9Document9 pagesB2B Project Proposal It Sector: Group 9Budhaditya BiswasNo ratings yet
- ETICS Fixings / E.W.IDocument54 pagesETICS Fixings / E.W.INarendra Reddy BhumaNo ratings yet
- Feasibility Study For Offshore Wind Farm Development in Tamil NaduDocument79 pagesFeasibility Study For Offshore Wind Farm Development in Tamil Nadujho elpeNo ratings yet
- Steritest System Brochure Br1495en MKDocument152 pagesSteritest System Brochure Br1495en MKmicro.labNo ratings yet
- Gabriela F. Sullivan: EducationDocument1 pageGabriela F. Sullivan: Educationapi-437973487No ratings yet
- 1.smart Light, Temperature, Air Condition ControlDocument4 pages1.smart Light, Temperature, Air Condition ControlFatin Nur Syahirah AzharNo ratings yet
- Impact of Climate Change On Floriculture and Landscape GardeningDocument38 pagesImpact of Climate Change On Floriculture and Landscape GardeningRuby SarmahNo ratings yet
- Herbicide and Formulation PDFDocument760 pagesHerbicide and Formulation PDFajengNo ratings yet
- IELTS Free Practice TestDocument22 pagesIELTS Free Practice TestKim MedairosNo ratings yet
- GRE Word List FDocument5 pagesGRE Word List FAnuj KaushikNo ratings yet
- PDF A Gentle Course in Local Class Field Theory Local Number Fields Brauer Groups Galois Cohomology 1St Edition Pierre Guillot Ebook Full ChapterDocument54 pagesPDF A Gentle Course in Local Class Field Theory Local Number Fields Brauer Groups Galois Cohomology 1St Edition Pierre Guillot Ebook Full Chapterdaphne.szymanski787100% (6)
- The Thai Spirit House: by Marisa Cranfill YoungDocument2 pagesThe Thai Spirit House: by Marisa Cranfill Youngsian017No ratings yet
- PL2303 G Series ManualDocument1 pagePL2303 G Series ManualGesiNo ratings yet
- UntitledDocument2 pagesUntitledSergey ShashminNo ratings yet
- A Broadband Planar Magic-T Using Microstrip-Slotline TransitionsDocument6 pagesA Broadband Planar Magic-T Using Microstrip-Slotline TransitionsSarvesh HireNo ratings yet
- MANUALESDocument84 pagesMANUALESPedroJose0% (1)
- Group1 OB Ward-Case StudyDocument10 pagesGroup1 OB Ward-Case StudyAnthony Seth AguilandoNo ratings yet