You might also like
- Acls 2023Document5 pagesAcls 2023Mohamed Helal100% (5)
- ACLS Pocket Card PDFDocument6 pagesACLS Pocket Card PDFdang vu hoang ducNo ratings yet
- Immediate Management of Major Postpartum Haemorrhage (PPH) : Call For HelpDocument1 pageImmediate Management of Major Postpartum Haemorrhage (PPH) : Call For HelpSALMA HANINA100% (1)
- Adult Cardiac Arrest Algorithm: VF/PVT Asystole/PEADocument8 pagesAdult Cardiac Arrest Algorithm: VF/PVT Asystole/PEAVitor Hugo100% (2)
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- ACLS 2015 Algorithm and Anesthesia ACLS PDFDocument14 pagesACLS 2015 Algorithm and Anesthesia ACLS PDFTaufiqurrahman RizkiNo ratings yet
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocument2 pagesStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaNo ratings yet
- Cardiac Arrest Circular AlgorhythmDocument4 pagesCardiac Arrest Circular AlgorhythmAisyah Nur KarimahNo ratings yet
- Cardiac Arrest Circular Algorithm: Start CPR 2 M IN UT ESDocument1 pageCardiac Arrest Circular Algorithm: Start CPR 2 M IN UT ESjohndoe1995No ratings yet
- Algo Pals Pediatric Cardiac ArrestDocument1 pageAlgo Pals Pediatric Cardiac Arrestpedjoang fkupr2017No ratings yet
- Cardiac Arrest Algorithm: Give OxygenDocument2 pagesCardiac Arrest Algorithm: Give OxygenJunius SimarmataNo ratings yet
- AclsDocument1 pageAclsJoice DasNo ratings yet
- Advance Life Support MaterialDocument2 pagesAdvance Life Support MaterialmayNo ratings yet
- Algorithms - Paediatric Advanced Life Support PDFDocument1 pageAlgorithms - Paediatric Advanced Life Support PDFLenox BlackNo ratings yet
- Algo Pals Pediatric Cardiac ArrestDocument1 pageAlgo Pals Pediatric Cardiac ArrestDevi ChrestellaNo ratings yet
- Reanimacion CardiopulmonarDocument15 pagesReanimacion CardiopulmonarVictoriano ValienteNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- 2-Cardiac Arrest AlgrthmDocument1 page2-Cardiac Arrest AlgrthmterminallllNo ratings yet
- Cardiac Arrest VF/Pulseless VT Learning Station ChecklistDocument5 pagesCardiac Arrest VF/Pulseless VT Learning Station ChecklistMaryam FadahNo ratings yet
- Shock: Shout For Help/Activate Emergency ResponseDocument6 pagesShock: Shout For Help/Activate Emergency ResponseandiyanimalikNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- Figure 4 AlgorithmACLS CACOVID 220101Document1 pageFigure 4 AlgorithmACLS CACOVID 220101AndhikaNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- Pediatric Cardiac Arrest Algorithm-2015 UpdateDocument2 pagesPediatric Cardiac Arrest Algorithm-2015 UpdateKholida UlfaNo ratings yet
- Adult Advanced Life Support Algorithm 2021 Aug 2023Document1 pageAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNo ratings yet
- Wa0000.Document7 pagesWa0000.benitez1228No ratings yet
- Acls Patient Algorithms: Greg Cook's Version of A Phoenix Fire DPT ClasicDocument4 pagesAcls Patient Algorithms: Greg Cook's Version of A Phoenix Fire DPT ClasicDouglas Greg CookNo ratings yet
- Adult Asystole or PeaDocument1 pageAdult Asystole or PeamayNo ratings yet
- Algorithms of AHA 2020Document23 pagesAlgorithms of AHA 2020Emirhan llkhanNo ratings yet
- Paediatric Advanced Life Support: Call For Help 2222 Commence/continue CPR (5 Initial Breaths Then CV Ratio 15:2)Document1 pagePaediatric Advanced Life Support: Call For Help 2222 Commence/continue CPR (5 Initial Breaths Then CV Ratio 15:2)Vijay RNo ratings yet
- ACLS Algorithms Adult 2010Document12 pagesACLS Algorithms Adult 2010anon_336736395No ratings yet
- Acls Algorithms 2012Document12 pagesAcls Algorithms 2012kivuNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanNo ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
- 8-Adult Advanced Life Support Algorithm 2021Document1 page8-Adult Advanced Life Support Algorithm 2021khaledNo ratings yet
- PalsalgoDocument1 pagePalsalgozacklim_2000No ratings yet
- AlgorithmACLSBradycardiawithapulse PDFDocument1 pageAlgorithmACLSBradycardiawithapulse PDFjohndoe1995No ratings yet
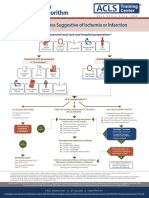
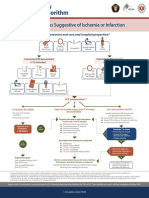
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Adenosine: Rapid IV PushDocument4 pagesAdenosine: Rapid IV PushsabboNo ratings yet
- Alsalgo PDFDocument1 pageAlsalgo PDFDelvanny Alfikri Rekaputri WicaksonoNo ratings yet
- AlsalgoDocument1 pageAlsalgozacklim_2000No ratings yet
- 3.ALS Algorithms Advanced Life SupportDocument1 page3.ALS Algorithms Advanced Life SupportLucian Alin DinuNo ratings yet
- Advanced Paediatric Life Support - A0 PDFDocument1 pageAdvanced Paediatric Life Support - A0 PDFiulia-uroNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Algorithm-ACLS CA 200731Document1 pageAlgorithm-ACLS CA 200731Hyunsoo EllisNo ratings yet
- Drug Main ACLS Use Dose/Route NotesDocument4 pagesDrug Main ACLS Use Dose/Route NotesshadyNo ratings yet
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- ACLS ReportDocument58 pagesACLS ReportCamille Honeyleith FernandoNo ratings yet
- Dopamine Drug StudyDocument3 pagesDopamine Drug StudyKwin Saludares100% (1)
- Endotracheal Intubation & ER Board Exam QuestionsDocument33 pagesEndotracheal Intubation & ER Board Exam QuestionsJo-Anne Karen Serdeña0% (1)
- Day Case Anaesthesia: Andrew Green MBBS, Fracgp GP Anaesthetist ANZCA RegistrarDocument50 pagesDay Case Anaesthesia: Andrew Green MBBS, Fracgp GP Anaesthetist ANZCA RegistrarSolape Akin-WilliamsNo ratings yet
- Ethico - Moral Responsibility of Nurses in Surgery: Ethical PrinciplesDocument9 pagesEthico - Moral Responsibility of Nurses in Surgery: Ethical PrinciplesClaire BatiaoNo ratings yet
- Examination of Gastrointestinal SystemDocument37 pagesExamination of Gastrointestinal SystemayushiNo ratings yet
- Veterinary AngiographyDocument37 pagesVeterinary AngiographyAmulyaVemulapadNo ratings yet
- Lohchab Nursing Home SlipDocument3 pagesLohchab Nursing Home SlipsalimNo ratings yet
- 201702030bEN Selectsecure 3830 Spec SheetDocument2 pages201702030bEN Selectsecure 3830 Spec SheetBian PurwaNo ratings yet
- UW - Fluoro ProtocolDocument57 pagesUW - Fluoro ProtocolIbrahim Mohammed Mohammed MorshedNo ratings yet
- Removal of Broken HardwareDocument8 pagesRemoval of Broken Hardwarecronoss21No ratings yet
- GroupC Baldaniya, Rajeshbhai PDFDocument16 pagesGroupC Baldaniya, Rajeshbhai PDFRajeshbhai Vinubhai BaldaniyaNo ratings yet
- Large Bowel ObstructionDocument36 pagesLarge Bowel Obstructionpuleng matshabaNo ratings yet
- HFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationDocument16 pagesHFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationflowlineNo ratings yet
- Principles Tendon Transfer - Omer 2004Document13 pagesPrinciples Tendon Transfer - Omer 2004Professeur Christian DumontierNo ratings yet
- Sterilization ConsentDocument20 pagesSterilization Consentyma9No ratings yet
- Cat Surg CatalogDocument80 pagesCat Surg CatalogPhilip McNelsonNo ratings yet
- Chapter 5 The Skeletal SystemDocument22 pagesChapter 5 The Skeletal SystemJUSTINE MAE MANTILLANo ratings yet
- AbdWall, Hernia Atbp - AnnoDocument34 pagesAbdWall, Hernia Atbp - AnnoJuan Lorenzo RequironNo ratings yet
- Synopsis 16-5-2023Document33 pagesSynopsis 16-5-2023Dr Danish NawazNo ratings yet
- Anatomy of HandDocument54 pagesAnatomy of Handromaisa akhtar100% (1)
- Neuroscience For Neurosurgeons Feb 29 2024 - 110883146X - Cambridge University Press 1St Edition Farhana Akter Full ChapterDocument68 pagesNeuroscience For Neurosurgeons Feb 29 2024 - 110883146X - Cambridge University Press 1St Edition Farhana Akter Full Chapterdale.freyer940100% (6)
- Operation Atlas of Hepato Pancreato Biliary Surgery Collected CaseDocument339 pagesOperation Atlas of Hepato Pancreato Biliary Surgery Collected Caseمحمد ورفليNo ratings yet
- Laser Hair Removal Treatment - Oliva ClinicDocument23 pagesLaser Hair Removal Treatment - Oliva Clinicolivaclinic100% (1)
- 09 Pulsar2 PDFDocument7 pages09 Pulsar2 PDFhelpurusNo ratings yet
- Cardio Pulmonary Resuscitation CPR PDFDocument6 pagesCardio Pulmonary Resuscitation CPR PDFKuldeep100% (1)
- English Project - Boomer YearsDocument14 pagesEnglish Project - Boomer YearsGushyNo ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Guidelines Gagal NafasDocument35 pagesGuidelines Gagal NafasRhevyNo ratings yet
- 16 OdtDocument2 pages16 OdtKHYATI PARMARNo ratings yet
- Parasagittal MeningiomaDocument51 pagesParasagittal MeningiomaAji Setia UtamaNo ratings yet
- Hydronephrosis OutlineDocument13 pagesHydronephrosis OutlineSarah Sy-SantosNo ratings yet