You might also like
- Drug StudyDocument7 pagesDrug StudyCheska Mae PalicNo ratings yet
- Micro K (Potassium Chloride)Document2 pagesMicro K (Potassium Chloride)ENo ratings yet
- Drug Study SummaryDocument7 pagesDrug Study SummaryKateLayaogNo ratings yet
- DS (Calcium + Vit. D)Document6 pagesDS (Calcium + Vit. D)Mary April MendezNo ratings yet
- Drug StudyDocument33 pagesDrug Studyjefwy8No ratings yet
- Lida AjocDocument10 pagesLida AjocEzra Knight Llesis AcebedoNo ratings yet
- Drug StudyDocument9 pagesDrug StudyKAROL MARIAE LUZ ERESNo ratings yet
- Drug Study (Med Ward Duty)Document6 pagesDrug Study (Med Ward Duty)Kimberly Abellar LatoNo ratings yet
- Drug Study (V.luna)Document4 pagesDrug Study (V.luna)carizzajoyNo ratings yet
- DRUGSTUDYDocument6 pagesDRUGSTUDYMauriceNo ratings yet
- Drug Study - LactuloseDocument2 pagesDrug Study - LactuloseCath Bril100% (1)
- Name of DrugsDocument3 pagesName of DrugsMiaLynn PangkuNo ratings yet
- Drug StudyDocument4 pagesDrug StudyMelody Forca FranciscoNo ratings yet
- Age Drug StudyDocument20 pagesAge Drug StudyLadybelle GototosNo ratings yet
- Drugstudy JRODDocument4 pagesDrugstudy JRODPeyjeyNo ratings yet
- CaCO3 Drug StudDocument2 pagesCaCO3 Drug StudAubrey SungaNo ratings yet
- Drug StudyDocument1 pageDrug Studyjasper pachingelNo ratings yet
- Print MeDocument4 pagesPrint MeDoneva Lyn MedinaNo ratings yet
- SOAP Pharm D HepaDocument13 pagesSOAP Pharm D HepaFatma HasanNo ratings yet
- Drug StudyDocument3 pagesDrug StudyRoscoe ParaanNo ratings yet
- SUMAOANG - Maalox Drug StudyDocument4 pagesSUMAOANG - Maalox Drug StudyMina SumaoangNo ratings yet
- Viii. Pharmacologic Intervention (Drug Study)Document10 pagesViii. Pharmacologic Intervention (Drug Study)Cyril Jane Caanyagan AcutNo ratings yet
- TELMISARTANDocument8 pagesTELMISARTANCidny CalimagNo ratings yet
- Zaroxolyn MetolazoneDocument1 pageZaroxolyn MetolazoneCassieNo ratings yet
- NCP DS NCM114 RleDocument12 pagesNCP DS NCM114 RleAllysa Kyle AlfonsoNo ratings yet
- Drug Study MsDocument10 pagesDrug Study MsAbie Jewel Joy RoqueNo ratings yet
- KaliumDocument2 pagesKaliumJustine Kaye Iballa HarligaNo ratings yet
- Chapter 5 Drug StudyDocument16 pagesChapter 5 Drug StudyRegee Rose LacsonNo ratings yet
- Drug StudyDocument32 pagesDrug StudyJoanne Bernadette Aguilar100% (1)
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- DRUG STUDY PesebreDocument3 pagesDRUG STUDY PesebreFrancoise Nicolette PesebreNo ratings yet
- UPDATES IN DIFFERENT COLORSDocument1 pageUPDATES IN DIFFERENT COLORSgeorgeloto12No ratings yet
- Brand Name: Generic Name: Stock Dose: Route: Frequency: ClassificationDocument4 pagesBrand Name: Generic Name: Stock Dose: Route: Frequency: ClassificationApril Joy MangsatNo ratings yet
- Losartan Drug Study for Acute Kidney FailureDocument3 pagesLosartan Drug Study for Acute Kidney FailureLouie Danielle SegarraNo ratings yet
- RandomDocument2 pagesRandomAllen YnionNo ratings yet
- Go KCLDocument7 pagesGo KCLSAMANTHA T. MODESTONo ratings yet
- Drug StudyDocument9 pagesDrug StudyComia AltheiaNo ratings yet
- Drug StudyDocument6 pagesDrug StudyKyle Margaret FloresNo ratings yet
- Drug Study (Ranitidine, Metoclopramide, Ketorolac, and Omeprazole)Document8 pagesDrug Study (Ranitidine, Metoclopramide, Ketorolac, and Omeprazole)Akisan0% (1)
- Calcium channel blocker and antacid drug studiesDocument28 pagesCalcium channel blocker and antacid drug studiessfkjalkhsafgNo ratings yet
- PHRM TemplateDocument4 pagesPHRM TemplateRichard SakyiamahNo ratings yet
- Drug StudyDocument4 pagesDrug StudyKaye Aligato ParaderoNo ratings yet
- Drug and Dietary Nursing ImplicationsDocument3 pagesDrug and Dietary Nursing ImplicationsFELICIA KASIMUNo ratings yet
- Potassium ChlorideDocument2 pagesPotassium ChlorideAdrianne BazoNo ratings yet
- Drug NameDocument9 pagesDrug NameJonathan MangawiliNo ratings yet
- Mechanism of Action, Indications, Contraindications, and Nursing Responsibilities for Magnesium SulfateDocument5 pagesMechanism of Action, Indications, Contraindications, and Nursing Responsibilities for Magnesium SulfateWestley RubinoNo ratings yet
- Kate Drug StudyDocument2 pagesKate Drug StudyShiehan Mae ForroNo ratings yet
- 13 Med MNGTDocument19 pages13 Med MNGTKate ChavezNo ratings yet
- Pharmacological Sheet Patient Name: BALDESTOY, Benedict Age: 19 Years Old Sex: Male Diagnosis: Hepatoma CAP-MRDocument5 pagesPharmacological Sheet Patient Name: BALDESTOY, Benedict Age: 19 Years Old Sex: Male Diagnosis: Hepatoma CAP-MRIngrid NicolasNo ratings yet
- Tugas DulcolaxDocument2 pagesTugas DulcolaxPriska Nagh Gas-oneNo ratings yet
- Drug Study HepatitisDocument7 pagesDrug Study Hepatitisjulesubayubay5428100% (1)
- Drug Study EntecavirDocument4 pagesDrug Study EntecavirClarimae AwingNo ratings yet
- Drug Study: Generic Name: Mechanism of ActionDocument9 pagesDrug Study: Generic Name: Mechanism of ActionSheferely BayauaNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Constipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationFrom EverandConstipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Diabetic Ketoacidosis Care Guideline EdDocument2 pagesDiabetic Ketoacidosis Care Guideline EdSeno Adi WicaksonoNo ratings yet
- DM 20 ItemsDocument4 pagesDM 20 ItemsDayanara TagaloguinNo ratings yet
- JBDS 02 DKA Guideline Amended v2 June 2021Document49 pagesJBDS 02 DKA Guideline Amended v2 June 2021yunica simanjuntakNo ratings yet
- Sign Symptoms Ketoacidosis DiabeticDocument4 pagesSign Symptoms Ketoacidosis DiabeticMatthew NathanielNo ratings yet
- Diabetes Mellitus in ChildrenDocument29 pagesDiabetes Mellitus in ChildrenwoldemariamNo ratings yet
- DM and Oncology Semi Finals QuizDocument15 pagesDM and Oncology Semi Finals QuizKaren mae alvarroNo ratings yet
- Diabetic Ketoacidosis Case StudyDocument6 pagesDiabetic Ketoacidosis Case StudyJohn AlcantaraNo ratings yet
- Diabetes AACE 2016Document30 pagesDiabetes AACE 2016Μιχάλης ΤερζάκηςNo ratings yet
- Predictive Factor of Ketoacidosis in Tyoe 1 Diabetes MelitusDocument6 pagesPredictive Factor of Ketoacidosis in Tyoe 1 Diabetes MelitusHilna ShalihaNo ratings yet
- Anesthesiology Case PresDocument26 pagesAnesthesiology Case PresNasrah N. MusaNo ratings yet
- Lab Tests For DM WRNDocument45 pagesLab Tests For DM WRNLiaApprilia Kartinii Cupcupcuap ElvenadoNo ratings yet
- Intensive Care - MCQs in Intensive Care Medicine For The Final FFICM, Bellchambers, 2015 PDFDocument342 pagesIntensive Care - MCQs in Intensive Care Medicine For The Final FFICM, Bellchambers, 2015 PDFAyman MustafaNo ratings yet
- Fluid and Electrolyte Therapy in Diabetic KetoacidosisDocument13 pagesFluid and Electrolyte Therapy in Diabetic KetoacidosisLohJNo ratings yet
- Nursing Care of Patients With Diabetes MellitusDocument43 pagesNursing Care of Patients With Diabetes MellitusRashida RuwaNo ratings yet
- Diabetic Ketoacidosis Case StudyDocument6 pagesDiabetic Ketoacidosis Case StudyHomework Ping100% (2)
- Free Nclex RN Study GuideDocument25 pagesFree Nclex RN Study GuideKatie Shortt100% (11)
- Diebetes MellitusDocument16 pagesDiebetes Mellitusbayiyitz0003No ratings yet
- Icu Adult and PaedsDocument2 pagesIcu Adult and PaedsPrashin RocharamNo ratings yet
- Management of DKA PresentationDocument46 pagesManagement of DKA PresentationMuhammed YesufNo ratings yet
- Empagliflozin (Jardiance) : National Drug MonographDocument16 pagesEmpagliflozin (Jardiance) : National Drug MonographSunil Murkikar (GM - PMI Quality Operations)No ratings yet
- RPN -Priority and Delegation Practice Test QuestionsDocument5 pagesRPN -Priority and Delegation Practice Test Questionsdaljit chahalNo ratings yet
- Common Pediatric Emergencies - A2Document46 pagesCommon Pediatric Emergencies - A2Ahmad JustNo ratings yet
- Euglycemic DkaDocument15 pagesEuglycemic DkaVemuri SrinivasNo ratings yet
- GDM Screening Test and ManagementDocument5 pagesGDM Screening Test and ManagementTan Yuet YangNo ratings yet
- PNLE Nursing Practice IV (RN Pedia)Document9 pagesPNLE Nursing Practice IV (RN Pedia)Ma. Dominique L. FacultadNo ratings yet
- Department of General Practice - Family MedicineDocument122 pagesDepartment of General Practice - Family Medicinesteven hkNo ratings yet
- HonkDocument22 pagesHonkSitta Grewo LiandarNo ratings yet
- Diabetes Tipo 1 MedscapeDocument69 pagesDiabetes Tipo 1 MedscapeJesús Evangelista GomerNo ratings yet
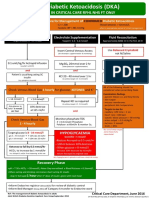
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocument1 pageAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNo ratings yet
- Cerebral EdemaDocument6 pagesCerebral EdemaantonopoulosalNo ratings yet