You might also like
- Florida School Grades 22Document55 pagesFlorida School Grades 22ABC Action News0% (2)
- LA Metro MapDocument1 pageLA Metro MapAlbert Barba0% (1)
- NSD With Iufd PathophysiologyDocument2 pagesNSD With Iufd Pathophysiologykaye040382% (11)
- The Pregnant AdolescentDocument15 pagesThe Pregnant Adolescentnursereview88% (8)
- A System of Urban/rural Typologies: Grid CellsDocument1 pageA System of Urban/rural Typologies: Grid CellsHajar AhmadNo ratings yet
- The Book Hill: SITEPLAN 1:1000Document2 pagesThe Book Hill: SITEPLAN 1:1000Victoria Solis PauwelsNo ratings yet
- Day 2 Morning Civ-Com CompleteDocument269 pagesDay 2 Morning Civ-Com CompletegbenjielizonNo ratings yet
- Montgomery County, Maryland 2001 Council DistrictsDocument1 pageMontgomery County, Maryland 2001 Council DistrictsM-NCPPCNo ratings yet
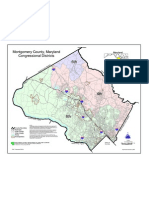
- Montgomery County, Maryland Congressional DistrictsDocument1 pageMontgomery County, Maryland Congressional DistrictsM-NCPPCNo ratings yet
- Montgomery County, Maryland Legislative DistrictsDocument1 pageMontgomery County, Maryland Legislative DistrictsM-NCPPCNo ratings yet
- The Indian ExpressDocument16 pagesThe Indian ExpressSiddhant GautamNo ratings yet
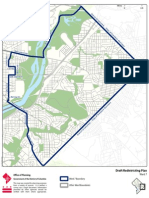
- DraftPlan 7Document1 pageDraftPlan 7CMMichaelABrownNo ratings yet
- Brosur IcalixDocument2 pagesBrosur Icalixdekymandiri77No ratings yet
- It's So Easy Going Green: An Interactive, Scientific Look at Protecting Our EnvironmentFrom EverandIt's So Easy Going Green: An Interactive, Scientific Look at Protecting Our EnvironmentNo ratings yet
- Graph: Equation StringDocument7 pagesGraph: Equation StringRahulNo ratings yet
- WFP 0000130513Document2 pagesWFP 0000130513h3493061No ratings yet
- JudgementDay-Clan Monster CodexDocument22 pagesJudgementDay-Clan Monster CodexRobert FcfNo ratings yet
- Dix BifDocument2 pagesDix Bifapi-26110262100% (1)
- New IGL BrochureDocument2 pagesNew IGL BrochureChun Chieh KeongNo ratings yet
- SP35 Plus Card Printer: Quick Install GuideDocument8 pagesSP35 Plus Card Printer: Quick Install GuidelftrevNo ratings yet
- Kyrgyzstan at Ten:: T I T "I D "Document47 pagesKyrgyzstan at Ten:: T I T "I D "somaliland_for_peaceNo ratings yet
- Letter Word Rec Error Analysis Form BDocument3 pagesLetter Word Rec Error Analysis Form BRoshni SondhiNo ratings yet
- TH C HànhDocument4 pagesTH C HànhLâm Thị Kiều AnhNo ratings yet
- 全身動脈圖表整理Document1 page全身動脈圖表整理irenesong922840053No ratings yet
- TP - M019 - M020 Section - 14,15,16Document1 pageTP - M019 - M020 Section - 14,15,16ON ROADING CONTRACTING LLCNo ratings yet
- Proposed Dealership Workshop for Granites and Concretes Limited & Spallette Enterprises LimitedDocument31 pagesProposed Dealership Workshop for Granites and Concretes Limited & Spallette Enterprises LimitedOluwaseyi JohnNo ratings yet
- AspirationsDocument10 pagesAspirationsdr satnam kaurNo ratings yet
- Leyline Scam Printable SB GuideDocument1 pageLeyline Scam Printable SB GuideRockfist7No ratings yet
- 11 Chart-RomansDocument2 pages11 Chart-RomansRafael Aleman100% (1)
- Montgomery County, Maryland Park Maintenance RegionsDocument1 pageMontgomery County, Maryland Park Maintenance RegionsM-NCPPCNo ratings yet
- Guide to snowboard widths for youth ridersDocument1 pageGuide to snowboard widths for youth ridersCNo ratings yet
- UVG 2E Grand Long Map - v100 Direttocut - Full MapDocument1 pageUVG 2E Grand Long Map - v100 Direttocut - Full MapArthur ViniciusNo ratings yet
- Animation Plan For EuropeDocument9 pagesAnimation Plan For EuroperepollorebeldeNo ratings yet
- Restorative Technique Selection in Class IV Direct Composite Restorations: A Simplified MethodDocument5 pagesRestorative Technique Selection in Class IV Direct Composite Restorations: A Simplified MethodCalisto GomesNo ratings yet
- Trend Map Shows New Business ModelsDocument1 pageTrend Map Shows New Business ModelsicavafNo ratings yet
- Global Bal G: Review I R V ViewDocument56 pagesGlobal Bal G: Review I R V ViewHarry ChristamaNo ratings yet
- Scan 31 Mar 2023Document2 pagesScan 31 Mar 2023Jayshree YadavNo ratings yet
- The State of Lagos Housing Market Report TEASERDocument29 pagesThe State of Lagos Housing Market Report TEASERDPX Digital NetworkNo ratings yet
- CH 12 Ribhu GitaDocument8 pagesCH 12 Ribhu Gitaime7No ratings yet
- Plascore SelectorhoneycombDocument1 pagePlascore SelectorhoneycombAryan PandeyNo ratings yet
- Crop Calendar: When to Plant Vegetables and FruitsDocument1 pageCrop Calendar: When to Plant Vegetables and FruitsAbrar AhmedNo ratings yet
- 1 Ankunft, Terminal 3 (Zugang) : Mazur ParkplatzDocument15 pages1 Ankunft, Terminal 3 (Zugang) : Mazur ParkplatzTijana SekulovNo ratings yet
- T G V NetworkDocument1 pageT G V Network9274No ratings yet
- Living River Charting Wetland Conditions of The Lower Santa Cruz River 2016 Water Year 1Document13 pagesLiving River Charting Wetland Conditions of The Lower Santa Cruz River 2016 Water Year 1KOLD News 13No ratings yet
- 025c45b5c3c0a5b6b2110c51e024f35627e7b1642b755d40760fd876e5cc9599_optimDocument3 pages025c45b5c3c0a5b6b2110c51e024f35627e7b1642b755d40760fd876e5cc9599_optimمنير الحديNo ratings yet
- Maturity Model Using KanbanDocument1 pageMaturity Model Using Kanbanmailtonoorul4114No ratings yet
- Recovered Acti Ve Deaths: Hospi Tal I ZedDocument1 pageRecovered Acti Ve Deaths: Hospi Tal I ZedWade ZhangNo ratings yet
- Marching Band Year Book Page 1Document2 pagesMarching Band Year Book Page 1api-549719383No ratings yet
- Regulator MapDocument1 pageRegulator MapJerNo ratings yet
- ChronostratChart2020 03Document1 pageChronostratChart2020 03JALAN KEBAIKANNo ratings yet
- Finitely Boring: Hanging Stay GradeDocument1 pageFinitely Boring: Hanging Stay GradeChayodom Vongbunsin TeeNo ratings yet
- Bogra Sub-Station Dimension MapDocument1 pageBogra Sub-Station Dimension Mapأون جهادNo ratings yet
- Theft From Motor Vehicle Maps For Aug. 19 To 25, 2019Document3 pagesTheft From Motor Vehicle Maps For Aug. 19 To 25, 2019Teresa VerencaNo ratings yet
- Passive Design Techniques and MaterialsDocument1 pagePassive Design Techniques and MaterialsTavneet SinghNo ratings yet
- 2018-19 Florida School GradesDocument59 pages2018-19 Florida School Grades10News WTSPNo ratings yet
- Tema 6 - Derivación DiscretaDocument5 pagesTema 6 - Derivación DiscretaLuyi WangNo ratings yet
- 2017.1 UPPSC Upper Pre 2017 - Paper - I - Answer - Key - (All - Sets)Document1 page2017.1 UPPSC Upper Pre 2017 - Paper - I - Answer - Key - (All - Sets)know oneNo ratings yet
- Reflected Ceiling Plan GDocument1 pageReflected Ceiling Plan Ghumaira fabihaNo ratings yet
- Hotel Management System With Online Environment For Hotel RivieraDocument49 pagesHotel Management System With Online Environment For Hotel RivieraSANTOSH VERMANo ratings yet
- ChangosDocument1 pageChangostenzo_xxNo ratings yet
- ChronostratChart2020 01Document1 pageChronostratChart2020 01Uang LanangNo ratings yet
- Map Airport RoutesDocument1 pageMap Airport RoutesJoe SimpsonNo ratings yet
- Salter Bab 06 General Principles PDFDocument26 pagesSalter Bab 06 General Principles PDFKahfi Rakhmadian KiraNo ratings yet
- Salter Chapter 5: Preceptor of Module Dr. Hermansyah, SpotDocument37 pagesSalter Chapter 5: Preceptor of Module Dr. Hermansyah, SpotKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Ca ParotisDocument15 pagesData Pasien Ca ParotisKahfi Rakhmadian KiraNo ratings yet
- Salter 15Document70 pagesSalter 15Kahfi Rakhmadian KiraNo ratings yet
- Orthopaedi FKUI RSCM 2008 GuideDocument22 pagesOrthopaedi FKUI RSCM 2008 Guiderandi_ciptaNo ratings yet
- Data Pasien Malignant Giant Cell RSUD ArifinDocument3 pagesData Pasien Malignant Giant Cell RSUD ArifinKahfi Rakhmadian KiraNo ratings yet
- Minimal Invasive Surgery, Robotic, Natural Orifice Transluminal EndoscopicDocument59 pagesMinimal Invasive Surgery, Robotic, Natural Orifice Transluminal EndoscopicKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Angio SarcomaDocument3 pagesData Pasien Angio SarcomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Malignant Giant Cell RSUD ArifinDocument3 pagesData Pasien Malignant Giant Cell RSUD ArifinKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Squamous Cell CaDocument27 pagesData Pasien Squamous Cell CaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien RabdomyosarcomaDocument12 pagesData Pasien RabdomyosarcomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Non Hodgkin LymphomaDocument25 pagesData Pasien Non Hodgkin LymphomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Ca PenisDocument3 pagesData Pasien Ca PenisKahfi Rakhmadian KiraNo ratings yet
- Data Pasien CA NasoparingDocument15 pagesData Pasien CA NasoparingKahfi Rakhmadian KiraNo ratings yet
- Data Pasien FibrosarcomaDocument9 pagesData Pasien FibrosarcomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Ca. TyroidDocument28 pagesData Pasien Ca. TyroidKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Ca. MamaeDocument1,013 pagesData Pasien Ca. MamaeKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Malignant FibrohistiocytomaDocument3 pagesData Pasien Malignant FibrohistiocytomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Ca ParotisDocument15 pagesData Pasien Ca ParotisKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Melanoma MalignaDocument3 pagesData Pasien Melanoma MalignaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien LiposarcomaDocument12 pagesData Pasien LiposarcomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Angio SarcomaDocument3 pagesData Pasien Angio SarcomaKahfi Rakhmadian KiraNo ratings yet
- Data Pasien CA NasoparingDocument15 pagesData Pasien CA NasoparingKahfi Rakhmadian KiraNo ratings yet
- Data Pasien CA NasoparingDocument15 pagesData Pasien CA NasoparingKahfi Rakhmadian KiraNo ratings yet
- Circulation 2015 Morrison S368 82Document16 pagesCirculation 2015 Morrison S368 82Kahfi Rakhmadian KiraNo ratings yet
- Data Pasien Ca PenisDocument3 pagesData Pasien Ca PenisKahfi Rakhmadian KiraNo ratings yet
- Data Pasien Adenoid Cysta CADocument3 pagesData Pasien Adenoid Cysta CAKahfi Rakhmadian KiraNo ratings yet
- Ventricular Tachycardia - Budi Baktijasa, MD, FIHA PDFDocument33 pagesVentricular Tachycardia - Budi Baktijasa, MD, FIHA PDFKahfi Rakhmadian KiraNo ratings yet
- Ajr 183 3 1830743Document8 pagesAjr 183 3 1830743Kahfi Rakhmadian KiraNo ratings yet
- Skill 08 (1) ..Blood Draw From A Central Venous CatheterDocument1 pageSkill 08 (1) ..Blood Draw From A Central Venous CatheternetsquadNo ratings yet
- Prelims Exam - (NCM 107)Document4 pagesPrelims Exam - (NCM 107)conahs nasugbu100% (1)
- Yearly Lesson Plan KSSM Science DLP Form 1 2021Document41 pagesYearly Lesson Plan KSSM Science DLP Form 1 2021RuddyMartini100% (1)
- Self-Medication and Safety Profile of Medicines Used Among Pregnant Women in A Tertiary Teaching Hospital in Jimma, Ethiopia: A Cross-Sectional StudyDocument15 pagesSelf-Medication and Safety Profile of Medicines Used Among Pregnant Women in A Tertiary Teaching Hospital in Jimma, Ethiopia: A Cross-Sectional StudyahmedNo ratings yet
- Radiology of Obstetrics and GynaecologyDocument61 pagesRadiology of Obstetrics and GynaecologyMUBIRU SAMUEL EDWARDNo ratings yet
- Psychological Changes of A Pregnant WomanDocument4 pagesPsychological Changes of A Pregnant WomanEuna Patricia AguilarNo ratings yet
- Screening and Diagnostic Test For Chromosomal DisordersDocument21 pagesScreening and Diagnostic Test For Chromosomal DisordersJohn Van Dave TaturoNo ratings yet
- Antenatal Assessment and Exercise DemonstrationDocument46 pagesAntenatal Assessment and Exercise DemonstrationPragati BholeNo ratings yet
- ToxichologyDocument36 pagesToxichologyWachi PampasNo ratings yet
- Phiq099 Physical Iq Afaa Prospectus 6Document15 pagesPhiq099 Physical Iq Afaa Prospectus 6tesfamichael100% (1)
- Acta Obstet Gynecol Scand - 2019 - Litwinska - Ventriculo Amniotic Shunting For Severe Fetal VentriculomegalyDocument6 pagesActa Obstet Gynecol Scand - 2019 - Litwinska - Ventriculo Amniotic Shunting For Severe Fetal VentriculomegalyApotik ApotekNo ratings yet
- Procedure: Case AnalysisDocument3 pagesProcedure: Case Analysisandreyou99No ratings yet
- Combiflam Tablets PI - 08072019Document13 pagesCombiflam Tablets PI - 08072019ArunNo ratings yet
- MCHN Midterm ReviewerDocument24 pagesMCHN Midterm Reviewerpat delapenaNo ratings yet
- School of Health and Allied Health Sciences Nursing DepartmentDocument2 pagesSchool of Health and Allied Health Sciences Nursing DepartmentJuviely PremacioNo ratings yet
- Surgical Conditions With Rocuronium Versus Suxamethonium in Cesarean Section: A Randomized TrialDocument8 pagesSurgical Conditions With Rocuronium Versus Suxamethonium in Cesarean Section: A Randomized TrialFadhilNo ratings yet
- Ob Set A and B QuesDocument17 pagesOb Set A and B QuesBok Delos SantosNo ratings yet
- Med Surg Bullets 1Document21 pagesMed Surg Bullets 1Jor GarciaNo ratings yet
- Intracardiac Echogenic Foci: Division of Maternal-Fetal Medicine & Fetal Cardiovascular MedicineDocument11 pagesIntracardiac Echogenic Foci: Division of Maternal-Fetal Medicine & Fetal Cardiovascular MedicineLuis LacsonNo ratings yet
- Neonatal Nutrition and Metabolism 2nd Ed. - P. Thureen, Et. Al., (Cambridge, 2006) WWDocument712 pagesNeonatal Nutrition and Metabolism 2nd Ed. - P. Thureen, Et. Al., (Cambridge, 2006) WWCampan Alina100% (1)
- BAHASA INGGRIS LITERASI MENGURANGI RISIKO KEHAMILANDocument6 pagesBAHASA INGGRIS LITERASI MENGURANGI RISIKO KEHAMILANHelmyHaikalNo ratings yet
- Maternal and Child Health NursingDocument73 pagesMaternal and Child Health NursingEcquin CapzyNo ratings yet
- Biology of Metabolism in Growing AnimalsDocument491 pagesBiology of Metabolism in Growing AnimalsFernando CruzNo ratings yet
- Karla RNC MSN Luxner Maternal Infant Nursing Care Plans 1999 PDFDocument321 pagesKarla RNC MSN Luxner Maternal Infant Nursing Care Plans 1999 PDFKen100% (1)
- 3 (OB Cases)Document267 pages3 (OB Cases)Sharyl Plan SarominesNo ratings yet
- Test Bank For Maternal Child Nursing Care 6th Edition by Perry DownloadDocument14 pagesTest Bank For Maternal Child Nursing Care 6th Edition by Perry Downloadkarenkingedmkptqajz100% (23)
- Reproduction QuestionsDocument16 pagesReproduction QuestionssalinaNo ratings yet
- MRSM SPM Trial 2009 Est Paper 2Document15 pagesMRSM SPM Trial 2009 Est Paper 2nursuhailahNo ratings yet
- (Michelle Murray PHD RNC) Antepartal and Intrapar (B-Ok - Xyz)Document249 pages(Michelle Murray PHD RNC) Antepartal and Intrapar (B-Ok - Xyz)Yo MeNo ratings yet