You might also like
- Ventricular TachycardiaDocument4 pagesVentricular TachycardiaDicky SaputraNo ratings yet
- Supraventricular TachycardiDocument8 pagesSupraventricular TachycardiHairunisa 0049No ratings yet
- Classification: Tachycardia Ventricles Heart Arrhythmia Ventricular Fibrillation Sudden Death EditDocument5 pagesClassification: Tachycardia Ventricles Heart Arrhythmia Ventricular Fibrillation Sudden Death EditConchita PepitaNo ratings yet
- Broad Complex Tachycardia-LatestDocument96 pagesBroad Complex Tachycardia-LatestEsayas KebedeNo ratings yet
- Ventricular TachycardiaDocument17 pagesVentricular TachycardiaAyu Rezki FadliyaNo ratings yet
- Ventricular Tachyarrhythmias: Roger D. White, M.DDocument2 pagesVentricular Tachyarrhythmias: Roger D. White, M.DEugene VovchukNo ratings yet
- Clinmed 23 5 442Document7 pagesClinmed 23 5 442Mey TalabessyNo ratings yet
- Lewis: Medical-Surgical Nursing, 8th Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - PrintableDocument6 pagesLewis: Medical-Surgical Nursing, 8th Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - Printablelpirman05No ratings yet
- Ventricular TachyarrythmiasDocument138 pagesVentricular TachyarrythmiasAbnet WondimuNo ratings yet
- Wide Qrs Tachy 2Document6 pagesWide Qrs Tachy 2Mohit TandonNo ratings yet
- Ventricular ArrhythmiaDocument37 pagesVentricular Arrhythmiaelhassia elhassiaNo ratings yet
- Incessant VT VFDocument9 pagesIncessant VT VFTor JaNo ratings yet
- Crisis Management of Cardiac Arrest in The ORDocument12 pagesCrisis Management of Cardiac Arrest in The ORANGELICANo ratings yet
- Heart Disease VDocument8 pagesHeart Disease VJOUBERT ALVAREZNo ratings yet
- ABC of Clinical Electrocardiography Myocardial IschaemiaDocument6 pagesABC of Clinical Electrocardiography Myocardial IschaemiaShri Mahalaxmi HarishNo ratings yet
- Supraventricular Tachycardia: An Overview of Diagnosis and ManagementDocument5 pagesSupraventricular Tachycardia: An Overview of Diagnosis and Managementanggit23No ratings yet
- Multiprofessional Critical Care Review Course - 2005Document16 pagesMultiprofessional Critical Care Review Course - 2005asupicuNo ratings yet
- Articulo 3Document12 pagesArticulo 3Andrea OrtizNo ratings yet
- Dysrhythmias Chapter 36Document6 pagesDysrhythmias Chapter 36Mahmoud KhelfaNo ratings yet
- Arritmias VentricularesDocument11 pagesArritmias VentricularesJesusIsmaelCoronaNo ratings yet
- 1 s2.0 S0749070421001020 MainDocument12 pages1 s2.0 S0749070421001020 MainEliseu AmaralNo ratings yet
- Wide QRS Complex Tachycardias - Causes, Epidemiology, and Clinical Manifestations - UpToDateDocument27 pagesWide QRS Complex Tachycardias - Causes, Epidemiology, and Clinical Manifestations - UpToDateNavkiran BhartiNo ratings yet
- ABC of Clinical Electrocardiography Broad Complex Tachycardia-Part IDocument4 pagesABC of Clinical Electrocardiography Broad Complex Tachycardia-Part IIgnacio Aguilar ValdiviesoNo ratings yet
- Answer NDocument1 pageAnswer NJ tanieeNo ratings yet
- touchCARDIO EJAE 7.1 pp04-11Document8 pagestouchCARDIO EJAE 7.1 pp04-11Carlos Navarro alonsoNo ratings yet
- Broad Complex TachyDocument8 pagesBroad Complex TachyarnabNo ratings yet
- Notes Before ExamDocument24 pagesNotes Before Exams2175183No ratings yet
- Pseudo-Myocardial Infarction Versus Pseudo-Pseudo-Myocardial InfarctionDocument3 pagesPseudo-Myocardial Infarction Versus Pseudo-Pseudo-Myocardial InfarctionAngel NspNo ratings yet
- R On T PhenomeneonDocument3 pagesR On T Phenomeneonpradeep danielNo ratings yet
- VT IndoDocument37 pagesVT IndotyaraNo ratings yet
- Arritmia SVDocument17 pagesArritmia SVCésar Lobo TarangoNo ratings yet
- NEONARYTDocument28 pagesNEONARYToctaviena zakariaNo ratings yet
- VT 2Document49 pagesVT 2Micija CucuNo ratings yet
- POSTER - CASE REPORT Ver.2 Ventricular Tachycardia Storm and Unstable Ventricular Tachycardia in A 48-Years-Old Man Following A Non-ST Elevation Myocardial InfarctionDocument1 pagePOSTER - CASE REPORT Ver.2 Ventricular Tachycardia Storm and Unstable Ventricular Tachycardia in A 48-Years-Old Man Following A Non-ST Elevation Myocardial InfarctionRJMNo ratings yet
- Junctional Ectopic Tachycardia in Infants and Children: Ranjit I. Kylat MD - Ricardo A. Samson MDDocument8 pagesJunctional Ectopic Tachycardia in Infants and Children: Ranjit I. Kylat MD - Ricardo A. Samson MDCatherine MorrisNo ratings yet
- Differentiate Between: Defibrillation CardioversionDocument3 pagesDifferentiate Between: Defibrillation CardioversionStephy SojanNo ratings yet
- 285 Perioperative Cardiac Dysrhythmias - Part 2 v2Document12 pages285 Perioperative Cardiac Dysrhythmias - Part 2 v2afid2912No ratings yet
- Evaluation of Supraventricular TachycardiaDocument11 pagesEvaluation of Supraventricular TachycardiaJazmín Alejandra AGNo ratings yet
- Richardson 1983Document5 pagesRichardson 1983adwaitsodaniNo ratings yet
- Crite RiosDocument8 pagesCrite RiosNilson Morales CordobaNo ratings yet
- 5 - Ventricular Tachyarrhythmias DoneDocument79 pages5 - Ventricular Tachyarrhythmias Doneclaimstudent3515No ratings yet
- Neo Pedia Guidelines Arrhythmia PDFDocument16 pagesNeo Pedia Guidelines Arrhythmia PDFkhludNo ratings yet
- Kalyanam Shivkumar Catheter Ablation of VentricularDocument10 pagesKalyanam Shivkumar Catheter Ablation of Ventricularrvp.180088No ratings yet
- Narrow QRS Complex Tachycardias: Clinical Manifestations, Diagnosis, and EvaluatDocument24 pagesNarrow QRS Complex Tachycardias: Clinical Manifestations, Diagnosis, and EvaluataspxxNo ratings yet
- ArrhythmiasDocument48 pagesArrhythmiasHarshan JeyakumarNo ratings yet
- JET2Document8 pagesJET2fufuka fukalifuNo ratings yet
- Ventricular Tachycardia: Dashboard Study Plans Library Qbank Analysis Account Help Center & Legal InfoDocument72 pagesVentricular Tachycardia: Dashboard Study Plans Library Qbank Analysis Account Help Center & Legal InfoNayla TasneemNo ratings yet
- SVT Mayo 2008Document12 pagesSVT Mayo 2008muhanasNo ratings yet
- Arritmias Ventriculares CecilDocument26 pagesArritmias Ventriculares CecilNestor Armando Tapia VelazcoNo ratings yet
- Cardiac LipomDocument4 pagesCardiac LipomCiprian MarianNo ratings yet
- Current Trends in Supraventricular Tachycardia Management: Daniel Sohinki, MD, Owen A. Obel, MDDocument10 pagesCurrent Trends in Supraventricular Tachycardia Management: Daniel Sohinki, MD, Owen A. Obel, MDAffandi HafidNo ratings yet
- Widecomplex Tachycardia: Mithilesh Kumar Das,, Archana Rajdev,, Vikas KalraDocument13 pagesWidecomplex Tachycardia: Mithilesh Kumar Das,, Archana Rajdev,, Vikas KalraTor JaNo ratings yet
- Nascimento Et Al. - 2013 - Wearable Cardioverter Defibrillator in Stress Cardiomyopathy and Cardiac ArrestDocument4 pagesNascimento Et Al. - 2013 - Wearable Cardioverter Defibrillator in Stress Cardiomyopathy and Cardiac ArrestflashjetNo ratings yet
- Pharmacological Treatment of ArrhytmiaDocument6 pagesPharmacological Treatment of ArrhytmiaLućia-Simona Perić ExOalđeNo ratings yet
- Nejmcps 2116690Document8 pagesNejmcps 2116690Luis MadrigalNo ratings yet
- Pathophysiology Week 1Document15 pagesPathophysiology Week 1Dan HoNo ratings yet
- Mujer Con Torsades de PointesDocument2 pagesMujer Con Torsades de PointesAníbal José Arroyo RodríguezNo ratings yet
- CHAPTER 123 TachyarrythmiasDocument7 pagesCHAPTER 123 TachyarrythmiasSandeep m rNo ratings yet
- BDG 2 Januari 2022Document2 pagesBDG 2 Januari 2022Sasya AndriansyahNo ratings yet
- BDG 1 Desember 2021Document1 pageBDG 1 Desember 2021Sasya AndriansyahNo ratings yet
- BABY STUFF (AutoRecovered)Document12 pagesBABY STUFF (AutoRecovered)Sasya AndriansyahNo ratings yet
- Form 2Document4 pagesForm 2Sasya AndriansyahNo ratings yet
- Hotel Uk Baru 5-8 MayDocument1 pageHotel Uk Baru 5-8 MaySasya AndriansyahNo ratings yet
- JadwalDocument1 pageJadwalSasya AndriansyahNo ratings yet
- Belakang Card MCDocument1 pageBelakang Card MCSasya AndriansyahNo ratings yet
- Surat Sponsor AnakDocument1 pageSurat Sponsor AnakSasya AndriansyahNo ratings yet
- Edition. Jakarta: EGC 2001.: Daftar PustakaDocument4 pagesEdition. Jakarta: EGC 2001.: Daftar PustakaSasya AndriansyahNo ratings yet
- Edition. Jakarta: EGC 2001.: Daftar PustakaDocument4 pagesEdition. Jakarta: EGC 2001.: Daftar PustakaSasya AndriansyahNo ratings yet
- Waltz of The FlowerDocument3 pagesWaltz of The FlowerSasya AndriansyahNo ratings yet
- NicardipineeeDocument8 pagesNicardipineeekevin100% (1)
- 10.1007@s11886 019 1213 XDocument13 pages10.1007@s11886 019 1213 XИлија РадосављевићNo ratings yet
- Hazel Hawkins Hospital Newsletter (Spring 2012)Document16 pagesHazel Hawkins Hospital Newsletter (Spring 2012)Fernando PerezNo ratings yet
- Ventricular Septal DefectDocument17 pagesVentricular Septal DefectWasim IqbalNo ratings yet
- Medical TerminologyDocument107 pagesMedical TerminologyonmcvNo ratings yet
- Advanced EKG RefresherDocument181 pagesAdvanced EKG RefresherIoana Antonesi100% (3)
- Mitral RegurgitationDocument10 pagesMitral RegurgitationWalter Saavedra YarlequeNo ratings yet
- Interventional Cardiac Electrophysiology - A Multidisciplinary Approach Section 1, Technology and Therapeutic Techniques - PDF RoomDocument306 pagesInterventional Cardiac Electrophysiology - A Multidisciplinary Approach Section 1, Technology and Therapeutic Techniques - PDF RoomVeronica JanethNo ratings yet
- This Study Resource Was: Silvestri: Saunders Comprehensive Review For The NCLEX-PN Examination, 7th EditionDocument4 pagesThis Study Resource Was: Silvestri: Saunders Comprehensive Review For The NCLEX-PN Examination, 7th EditionNeoGellinNo ratings yet
- Lead GenerationDocument9 pagesLead GenerationMuddaserNo ratings yet
- Bprints MEDICINE Best Copy SearchableDocument90 pagesBprints MEDICINE Best Copy SearchablePhilippe Ceasar BascoNo ratings yet
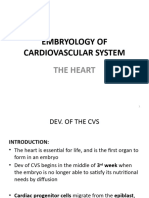
- Embryology of Cardiovascular System-1Document59 pagesEmbryology of Cardiovascular System-1bomabenediNo ratings yet
- Amiodarone and Lidocaine For The Treatment 1 1Document11 pagesAmiodarone and Lidocaine For The Treatment 1 1vanniNo ratings yet
- Arrow ACAT1 Intra Aortic Balloon Pump System Service ManualDocument221 pagesArrow ACAT1 Intra Aortic Balloon Pump System Service ManualFrank Quitian67% (3)
- Pathophysiology and Natural History of Atrial Septal DefectDocument10 pagesPathophysiology and Natural History of Atrial Septal DefectrosaNo ratings yet
- DIAG Y MANEJO TerapéuticoDocument12 pagesDIAG Y MANEJO TerapéuticoCORONARIA QUILMESNo ratings yet
- Hospital Case Study Max S.SDocument8 pagesHospital Case Study Max S.SIqRa JaVedNo ratings yet
- 3 - Cine TrainingDocument25 pages3 - Cine TrainingYonatan Merchant PerezNo ratings yet
- Perhitungan Kuda-Kuda Kayu Bentang 3m - RevisiDocument33 pagesPerhitungan Kuda-Kuda Kayu Bentang 3m - RevisideviNo ratings yet
- Congestive Cardiac FailureDocument45 pagesCongestive Cardiac FailureEndla SriniNo ratings yet
- EcgDocument18 pagesEcgDelyn Gamutan MillanNo ratings yet
- Lapkas JantungDocument25 pagesLapkas JantungJuwita Valen RamadhanniaNo ratings yet
- Factores para FNRDocument10 pagesFactores para FNRPOMYNo ratings yet
- Ecg Made Ridiculously Easy!Document78 pagesEcg Made Ridiculously Easy!momobelle100% (9)
- Emergency Medicine Mcqs Exam 2010-2011Document4 pagesEmergency Medicine Mcqs Exam 2010-2011Adam Adamako100% (4)
- Ecg PresentationDocument42 pagesEcg PresentationAnwar SiddiquiNo ratings yet
- SCAI Shock Classification DeckDocument22 pagesSCAI Shock Classification DeckJimmy JimmyNo ratings yet
- Brain Natriuretic PeptideDocument9 pagesBrain Natriuretic PeptideRio Kristian NugrohoNo ratings yet
- Journal On HIEDocument19 pagesJournal On HIEMohammad Misbahul IslamNo ratings yet
- ICU-ED Clinical AssignmentDocument5 pagesICU-ED Clinical AssignmentMark LiebNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)