You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- UMMP Guidelines For ExaminationDocument28 pagesUMMP Guidelines For ExaminationayuniNo ratings yet
- CPG Management of Bipolar Disorder in AdultsDocument78 pagesCPG Management of Bipolar Disorder in AdultsElvis NgNo ratings yet
- Chest X RAY: Airway and MediastinumDocument2 pagesChest X RAY: Airway and MediastinumayuniNo ratings yet
- Urological History TakingDocument6 pagesUrological History TakingayuniNo ratings yet
- PPD DR YungDocument1 pagePPD DR YungayuniNo ratings yet
- NAC Medications Chart 2016 A2Document1 pageNAC Medications Chart 2016 A2ayuniNo ratings yet
- Dysmorphic Syndromes - Thong Meow KeongDocument53 pagesDysmorphic Syndromes - Thong Meow KeongayuniNo ratings yet
- Procedural Skill Printout SurgeryDocument3 pagesProcedural Skill Printout SurgeryayuniNo ratings yet
- Attitude Evaluation Form - 30august2017Document1 pageAttitude Evaluation Form - 30august2017ayuniNo ratings yet
- Attitude Evaluation For Stage 3.1Document1 pageAttitude Evaluation For Stage 3.1ayuniNo ratings yet
- AppendicitisDocument11 pagesAppendicitisayuniNo ratings yet
- Reading and Writing Ophthalmology NotesDocument8 pagesReading and Writing Ophthalmology NotesayuniNo ratings yet
- Ear DischargeDocument23 pagesEar DischargeayuniNo ratings yet
- Rhinitis: by KhairunnisaDocument40 pagesRhinitis: by KhairunnisaayuniNo ratings yet
- A Tribute To Justice James Aaron Makau ArticleDocument4 pagesA Tribute To Justice James Aaron Makau ArticleMiracle O MudeyiNo ratings yet
- Overview of Iso 31000 Iso-Iec 31010 & Iso Guide 73Document54 pagesOverview of Iso 31000 Iso-Iec 31010 & Iso Guide 73pcstorecenter100% (2)
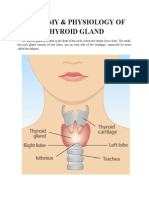
- Anatomy & Physiology of Thyroid GlandDocument5 pagesAnatomy & Physiology of Thyroid GlandJohnpaul DelapenaNo ratings yet
- Garbage In, Garbage OutDocument14 pagesGarbage In, Garbage OutPoonamNo ratings yet
- Applications of PCRDocument11 pagesApplications of PCRMustafa KhandgawiNo ratings yet
- Clinical Study of Bleaching Gel Storage Temperature On Tooth Color and SensitivityDocument10 pagesClinical Study of Bleaching Gel Storage Temperature On Tooth Color and SensitivityKhusnul Fatimah AzzahraNo ratings yet
- Neonatal Jaundice NICEDocument54 pagesNeonatal Jaundice NICEkyawswakyawswaNo ratings yet
- Skeletal and Muscular SystemDocument118 pagesSkeletal and Muscular SystemMark Kevin AguilarNo ratings yet
- Internal HSE Audit ProcedureDocument5 pagesInternal HSE Audit ProcedureGOWRI M MNo ratings yet
- Assignment 1 - Youmna Shatila 201600543Document5 pagesAssignment 1 - Youmna Shatila 201600543Youmna ShatilaNo ratings yet
- Biological BeginningsDocument13 pagesBiological BeginningsAmelinda MarmolNo ratings yet
- Obat Prekursor Dan OOTDocument7 pagesObat Prekursor Dan OOTAbdul kadir100% (1)
- Drug Study Hepa BDocument3 pagesDrug Study Hepa BKwebblekop JordiNo ratings yet
- Congenital Infiltrating Lipomatosis of The Face Case Report PDFDocument4 pagesCongenital Infiltrating Lipomatosis of The Face Case Report PDFfeli2010No ratings yet
- Physical Education and Health 2nd Sem Notes 12Document2 pagesPhysical Education and Health 2nd Sem Notes 12karilesbackupaccNo ratings yet
- 2011 Conference Book FinalDocument44 pages2011 Conference Book FinalIBWC1609No ratings yet
- The Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsDocument8 pagesThe Ertl Osteomyoplastic Amputation: History, Philosophy, Misconceptions, MisapplicationsanujNo ratings yet
- CDP Assessment ToolDocument20 pagesCDP Assessment ToolDilg Rizal Province0% (1)
- JollyDocument39 pagesJollysalmanNo ratings yet
- Health Strategy: PTI's Health VisionDocument67 pagesHealth Strategy: PTI's Health VisionPTI Official100% (14)
- Step 2Document64 pagesStep 2Irfan MajeedNo ratings yet
- Job Roles in The TV and Film Industry 2Document5 pagesJob Roles in The TV and Film Industry 2JackReeveNo ratings yet
- Conditii de Aparitie (Factori Declansatori)Document15 pagesConditii de Aparitie (Factori Declansatori)Roxana EnachescuNo ratings yet
- Changes That HealDocument3 pagesChanges That HealLight Learning ClubNo ratings yet
- Clinical Tests in Shoulder Examination - How To Perform ThemDocument7 pagesClinical Tests in Shoulder Examination - How To Perform ThemkabshielNo ratings yet
- Mapeh 8 1st Summative TestDocument5 pagesMapeh 8 1st Summative TestHezel Mercado Edrozo100% (2)
- Disaster Management and Nurses RoleDocument27 pagesDisaster Management and Nurses RolesweetpeaNo ratings yet
- FearandFashionFull Evaluation Report PDFDocument32 pagesFearandFashionFull Evaluation Report PDFTinaStiffNo ratings yet
- PNP PDSDocument5 pagesPNP PDSErlindo Bulaoat Jr.No ratings yet