You might also like
- Lean Muscle ProgramDocument2 pagesLean Muscle ProgramtonypodmoreNo ratings yet
- Foods That Burn Fat, Foods That Turn To Fat, Part 1Document8 pagesFoods That Burn Fat, Foods That Turn To Fat, Part 1S SPEEDNo ratings yet
- Strong Bodies, Strong Business: A Step-By-Step Guide to Building a Sustainable Business Through WeightliftingFrom EverandStrong Bodies, Strong Business: A Step-By-Step Guide to Building a Sustainable Business Through WeightliftingNo ratings yet
- Personal Training Agreement (Legal)Document1 pagePersonal Training Agreement (Legal)JoshMatthewsNo ratings yet
- Knee Rehab Tubing ExercisesDocument10 pagesKnee Rehab Tubing ExercisesRiana Khairani100% (1)
- Liebenson - Functional Training Handbook ReviewDocument3 pagesLiebenson - Functional Training Handbook ReviewJoaoPncs SilvaNo ratings yet
- Nutrition To Improve Your RunningDocument4 pagesNutrition To Improve Your RunningMichelle MontielNo ratings yet
- Foam Rolling GuideDocument14 pagesFoam Rolling GuideMariaNo ratings yet
- BosuDocument14 pagesBosuKarla Alzenda Cruzeiro100% (1)
- The Tabata Cardio WorkoutDocument2 pagesThe Tabata Cardio Workoutrogerlee2250No ratings yet
- ACS - Accelerated Corrective Strategies: Exercise GuideDocument1 pageACS - Accelerated Corrective Strategies: Exercise GuideAlastair HarrisNo ratings yet
- Corrective TrainingDocument5 pagesCorrective TrainingRazzyDazNo ratings yet
- The Runner's Building BlocksDocument39 pagesThe Runner's Building BlocksWaseela AdamNo ratings yet
- Fitness TRX Rip Trainers EspDocument1 pageFitness TRX Rip Trainers EspAntonioNo ratings yet
- Abdominal Strain Injury AKADocument31 pagesAbdominal Strain Injury AKAtony whartonNo ratings yet
- 12 The-Performance-Digest-Issue-12-September-17Document27 pages12 The-Performance-Digest-Issue-12-September-17Soylo Amado Rubio100% (1)
- SP Thirty Day Program Guide Apr2019 Grey FINDocument85 pagesSP Thirty Day Program Guide Apr2019 Grey FINLarissa100% (1)
- Getting Leaner: Introduction To HypertrophyDocument1 pageGetting Leaner: Introduction To Hypertrophyjole000No ratings yet
- Intermediate Level Strength Training Program1Document2 pagesIntermediate Level Strength Training Program1Dân Nguyễn100% (1)
- PAR Q AcsmDocument2 pagesPAR Q Acsmboltu100% (2)
- Top Sport Nutrition Myth PDFDocument2 pagesTop Sport Nutrition Myth PDFManuel FerreiraNo ratings yet
- ResistanceDocument32 pagesResistancedamned2No ratings yet
- P90X3 Elite Block Workout CalendarDocument2 pagesP90X3 Elite Block Workout CalendarDattathreya MunirathnamNo ratings yet
- The Female Athlete TriadDocument2 pagesThe Female Athlete Triadapi-298014898No ratings yet
- Basic Workout POWER PLATEDocument1 pageBasic Workout POWER PLATEBEecul ClauNo ratings yet
- GeneralistDocument19 pagesGeneralistRyan100% (1)
- Success Guide PDFDocument35 pagesSuccess Guide PDFDilip sayamNo ratings yet
- Hamstring Rehab Exercise GuidelinesDocument2 pagesHamstring Rehab Exercise Guidelineslouis1973No ratings yet
- 0021552785623322566322katie Corio Plyo Ebook PDFDocument7 pages0021552785623322566322katie Corio Plyo Ebook PDFDiana AlexandraNo ratings yet
- CrossFit Macro CalculatorDocument4 pagesCrossFit Macro CalculatorEmanuelNo ratings yet
- Rings 1 Getting Started GuideDocument13 pagesRings 1 Getting Started GuidedraguNo ratings yet
- TrainingmistakesDocument6 pagesTrainingmistakesrontraubNo ratings yet
- Muscle Gain Math - BodyrecompositionDocument3 pagesMuscle Gain Math - BodyrecompositionFake100% (1)
- Nutrition and Sports PerformanceDocument29 pagesNutrition and Sports PerformanceMomenHamedNo ratings yet
- Running GuideDocument10 pagesRunning Guidemishka1230% (1)
- Qi Yoga For Runners 20minDocument3 pagesQi Yoga For Runners 20mintikomioNo ratings yet
- Posechart Hip ChallengeDocument45 pagesPosechart Hip ChallengeDavid WilliamsNo ratings yet
- The Complete Jason Blaha Ice Cream Fitness 5x5 NoviceProgramDocument11 pagesThe Complete Jason Blaha Ice Cream Fitness 5x5 NoviceProgramgastaoNo ratings yet
- BodyBoss Exercises Alternatives To MachinesDocument4 pagesBodyBoss Exercises Alternatives To Machinesgdede95No ratings yet
- Henselmans Coaching Client Intake FormDocument10 pagesHenselmans Coaching Client Intake FormVarun kaushikNo ratings yet
- 4 Essential Strategies For The Correction of Anterior Pelvic TiltDocument10 pages4 Essential Strategies For The Correction of Anterior Pelvic TiltAlexander NarváezNo ratings yet
- BENCH BIBLE-Ultimate Frisbee Training ProgramDocument15 pagesBENCH BIBLE-Ultimate Frisbee Training ProgramalexNo ratings yet
- Basic Physical AbilitiesDocument5 pagesBasic Physical Abilitiesrumedv100% (1)
- Muscle: Women's Advanced Strength Training Workout RoutineDocument13 pagesMuscle: Women's Advanced Strength Training Workout Routineamey patkarNo ratings yet
- Fitness Leader's HandbookDocument623 pagesFitness Leader's HandbookRaviNo ratings yet
- Short Term Effects of Complex and ContrastDocument6 pagesShort Term Effects of Complex and ContrastKoordinacijska Lestev Speed LadderNo ratings yet
- Highy Effective Roll and ReleaseDocument20 pagesHighy Effective Roll and ReleaseHà Minh NguyệtNo ratings yet
- PT Course Manual 07 Functional - AssessmentsDocument87 pagesPT Course Manual 07 Functional - AssessmentsLouis TrầnNo ratings yet
- At-Home Workouts and Resources For Health and Fitness ProfessionalsDocument8 pagesAt-Home Workouts and Resources For Health and Fitness ProfessionalsNury QuintanarNo ratings yet
- Groin Strain Rehabilitation PDFDocument3 pagesGroin Strain Rehabilitation PDFOscar NgNo ratings yet
- CCMI Practitioner Course Itinerary 1Document1 pageCCMI Practitioner Course Itinerary 1dan iacobNo ratings yet
- Critical Analysis of Crossfit Within The Health and Fitness IndustryDocument23 pagesCritical Analysis of Crossfit Within The Health and Fitness IndustrySajeel ChaudhryNo ratings yet
- WODDocument8 pagesWODCarlos Alberto AcevedoNo ratings yet
- ACE Group Fitness Instructor University Curriculum: Chapter 3: Group Exercise Program DesignDocument20 pagesACE Group Fitness Instructor University Curriculum: Chapter 3: Group Exercise Program DesignLouis TrầnNo ratings yet
- 100 Yoga Poses For Home PDFDocument55 pages100 Yoga Poses For Home PDFSuosuo Lo0% (1)
- CV Personal TrainerDocument1 pageCV Personal TrainerAdrián Torres GonzálezNo ratings yet
- 30 Minute WorkoutDocument14 pages30 Minute WorkoutIordan FlorinNo ratings yet
- CEBM Levels of Evidence 2.1Document1 pageCEBM Levels of Evidence 2.1Béla TóthNo ratings yet
- Pharmaceutical Organisation Sructure and Functions AccDocument3 pagesPharmaceutical Organisation Sructure and Functions AccSelimHachichaNo ratings yet
- Value Education & Ehics Unit IDocument26 pagesValue Education & Ehics Unit IchanduNo ratings yet
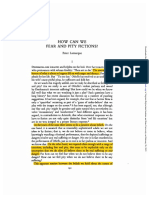
- Howcanwe Fear and Pity Fictions?: Peter LamarqueDocument14 pagesHowcanwe Fear and Pity Fictions?: Peter LamarqueAurora QuiterioNo ratings yet
- Learning Styles: Honey and Mumford: Sutton Coldfield College Action Research ProposalDocument17 pagesLearning Styles: Honey and Mumford: Sutton Coldfield College Action Research ProposalwauhahahaNo ratings yet
- Job Analysis and Job Description: Seema Singh, KUSOM, 2013Document15 pagesJob Analysis and Job Description: Seema Singh, KUSOM, 2013navin9849No ratings yet
- Disusun Untuk Memenuhi Sebagian Persyaratan Mencapai Gelar Sarjana KeperawatanDocument11 pagesDisusun Untuk Memenuhi Sebagian Persyaratan Mencapai Gelar Sarjana Keperawatansyahrul aulNo ratings yet
- Paper: 13:, Organization Behaviour, Motivation: Content TheoriesDocument15 pagesPaper: 13:, Organization Behaviour, Motivation: Content TheoriesABHINAV DEWALIYA100% (1)
- Summary of Crucial ConversationsDocument8 pagesSummary of Crucial ConversationsteynxmNo ratings yet
- Probability ExamplesDocument2 pagesProbability ExamplesSajjadNo ratings yet
- VervainDocument10 pagesVervainSundar Rajan100% (1)
- Asking and Giving OpinionDocument15 pagesAsking and Giving OpinionAvillNo ratings yet
- Audit of The Management of Call Centre OperationsDocument20 pagesAudit of The Management of Call Centre OperationsFrancis NyanguwoNo ratings yet
- Social Media Evaluation Aljay Keila KezzyDocument5 pagesSocial Media Evaluation Aljay Keila Kezzyapi-384500140No ratings yet
- Diversity As A Competitive Strategy in The Workplace: Dahlia D. Cunningham Daryl D. GreenDocument5 pagesDiversity As A Competitive Strategy in The Workplace: Dahlia D. Cunningham Daryl D. GreenmurkyNo ratings yet
- Abstracts Posters SatDocument58 pagesAbstracts Posters SatDiana RidicNo ratings yet
- Negotiation Skills: Presented By: Tanvi Abbott Tamanna Godara Priya Jain Sheena Jain Ritika Mehta Shalaka TiwariDocument29 pagesNegotiation Skills: Presented By: Tanvi Abbott Tamanna Godara Priya Jain Sheena Jain Ritika Mehta Shalaka TiwaritmnjulyNo ratings yet
- Course 5 Chapter 3 Section D. READING - Revisión Del IntentoDocument5 pagesCourse 5 Chapter 3 Section D. READING - Revisión Del IntentoDaniel SipacNo ratings yet
- Content AnalysisDocument18 pagesContent AnalysisTanvi Sharma50% (2)
- HarrassmentDocument41 pagesHarrassmentjippidionNo ratings yet
- Think Psychology 2Nd Edition Baird Test Bank Full Chapter PDFDocument49 pagesThink Psychology 2Nd Edition Baird Test Bank Full Chapter PDFLeslieBuchanannjfy100% (8)
- Use Your Own EyesDocument110 pagesUse Your Own EyesachublrNo ratings yet
- (Cambridge Ielts 1) Practice Test 1 - KeyDocument3 pages(Cambridge Ielts 1) Practice Test 1 - KeyAngie Nguyen100% (1)
- Useful Business English Phrases For MeetingsDocument15 pagesUseful Business English Phrases For Meetingsmagdazavala100% (2)
- Araujo Freedom and Dependency in Christian PartnershipsDocument6 pagesAraujo Freedom and Dependency in Christian PartnershipsTimothyHallsNo ratings yet
- Recollections: by David Christie MurrayDocument124 pagesRecollections: by David Christie MurrayGutenberg.orgNo ratings yet
- 11 - Blis Course Des PDFDocument2 pages11 - Blis Course Des PDFcnNo ratings yet
- A Modern Approach To Verbal and Non Verbal ReasoningDocument1,176 pagesA Modern Approach To Verbal and Non Verbal ReasoningSaif Sidd80% (5)
- Tinimbang Ka Ngunit KulangDocument4 pagesTinimbang Ka Ngunit KulangSighlene Baloran100% (1)
- Business CommunicationDocument8 pagesBusiness CommunicationDivyanand JhaNo ratings yet
- The 7 Habits of Highly Effective People: The Infographics EditionFrom EverandThe 7 Habits of Highly Effective People: The Infographics EditionRating: 4 out of 5 stars4/5 (2475)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (2)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (5)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Love Yourself, Heal Your Life Workbook (Insight Guide)From EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Rating: 5 out of 5 stars5/5 (40)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- The Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayFrom EverandThe Noom Kitchen: 100 Healthy, Delicious, Flexible Recipes for Every DayNo ratings yet
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Roadmap: Second Edition: The Get-It-Together Guide for Figuring Out What To Do with Your Life (Career Change Advice Book, Self Help Job Workbook)From EverandRoadmap: Second Edition: The Get-It-Together Guide for Figuring Out What To Do with Your Life (Career Change Advice Book, Self Help Job Workbook)Rating: 5 out of 5 stars5/5 (8)
- Eat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthFrom EverandEat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthRating: 2 out of 5 stars2/5 (1)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsFrom EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsRating: 5 out of 5 stars5/5 (7)
- Ultrametabolism: The Simple Plan for Automatic Weight LossFrom EverandUltrametabolism: The Simple Plan for Automatic Weight LossRating: 4.5 out of 5 stars4.5/5 (28)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (352)