You might also like
- Bit by Bit: Social Research in the Digital AgeFrom EverandBit by Bit: Social Research in the Digital AgeRating: 4 out of 5 stars4/5 (1)
- Soc 621 Final PaperDocument16 pagesSoc 621 Final Paperapi-478028340No ratings yet
- Additional TRF FormDocument1 pageAdditional TRF FormMINH NGUYỄN PHAN DUYNo ratings yet
- Application For Sending Original Test Report Form (TRF) HomeDocument1 pageApplication For Sending Original Test Report Form (TRF) HomeNguyễn Đức MạnhNo ratings yet
- International ESOL ApplicationDocument4 pagesInternational ESOL ApplicationNatalia Hernán-WaleckaNo ratings yet
- Format of Application For C Adm O, Air Force Station, .....................................................Document3 pagesFormat of Application For C Adm O, Air Force Station, .....................................................Sunil RAYALASEEMA GRAPHICSNo ratings yet
- Admission FormDocument1 pageAdmission FormYasin AhmedNo ratings yet
- Additional TRF Form (Loss or Damage)Document1 pageAdditional TRF Form (Loss or Damage)SunnyNo ratings yet
- Application For Sending Additional Test Report Form (TRF) : For Office Use OnlyDocument1 pageApplication For Sending Additional Test Report Form (TRF) : For Office Use Onlylinh nguyenNo ratings yet
- At StageDocument1 pageAt Stageky147245No ratings yet
- Universiti Teknikal Malaysia Melaka: Fakulti Teknologi Maklumat Dan KomunikasiDocument2 pagesUniversiti Teknikal Malaysia Melaka: Fakulti Teknologi Maklumat Dan KomunikasiSiti Nur Azrreen RuslanNo ratings yet
- Contractual Recruitment FormatDocument3 pagesContractual Recruitment FormatDhanjyoti NathNo ratings yet
- Alumni Form - UUM Convocation 2016 PDFDocument1 pageAlumni Form - UUM Convocation 2016 PDFAnonymous TgpPUaKNo ratings yet
- Application Form: Student Exchange Program (For Outbound Students)Document5 pagesApplication Form: Student Exchange Program (For Outbound Students)giang123No ratings yet
- GP Personal Details of StudentDocument2 pagesGP Personal Details of StudentNitin malikNo ratings yet
- Trinity Online Application FormDocument2 pagesTrinity Online Application FormNatalia Hernán-WaleckaNo ratings yet
- Application Form Sac PDFDocument7 pagesApplication Form Sac PDFdasunwk4No ratings yet
- Tracer Study Questionnaire: Kgyanwali@tcioe - Edu.npDocument3 pagesTracer Study Questionnaire: Kgyanwali@tcioe - Edu.npKR BhattaNo ratings yet
- UPDATED Scholarship Loan Form 2Document5 pagesUPDATED Scholarship Loan Form 2Ira CezanneNo ratings yet
- Application-Form-Teaching in The UniversityDocument4 pagesApplication-Form-Teaching in The UniversityAlex Obeng Asare100% (1)
- Application Form and Admit Card 2023Document3 pagesApplication Form and Admit Card 2023Roy KoushaniNo ratings yet
- 2024 Bursary in Take ApplicationDocument8 pages2024 Bursary in Take Applicationmakumenaledi03No ratings yet
- Meeting FormDocument2 pagesMeeting FormZubair GhaznaviNo ratings yet
- 7 - Tracer Study Form For Graduates (FINAL)Document6 pages7 - Tracer Study Form For Graduates (FINAL)Kia AdionNo ratings yet
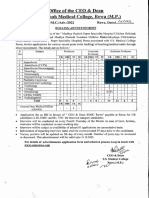
- Advt Medical Teachers GDMODocument4 pagesAdvt Medical Teachers GDMOravi SinghNo ratings yet
- Erasmus Mundus Joint Master Degree in Smart Cities and Communities (Smaccs)Document1 pageErasmus Mundus Joint Master Degree in Smart Cities and Communities (Smaccs)harisNo ratings yet
- Banasthali Vidyapith: PostDocument3 pagesBanasthali Vidyapith: PostTarunNo ratings yet
- Offline Application Form 2023 1Document2 pagesOffline Application Form 2023 1neelamenggcorp4667No ratings yet
- The Odisha Sch. Caste & Sch. Tribe Development Finance Co-Operative Corporation LimitedDocument3 pagesThe Odisha Sch. Caste & Sch. Tribe Development Finance Co-Operative Corporation LimitedDebasish GochhayatNo ratings yet
- Application Form in English For ProspectsDocument6 pagesApplication Form in English For ProspectsEzra LindholmNo ratings yet
- International English Language Testing System: Writing Answer SheetDocument4 pagesInternational English Language Testing System: Writing Answer Sheetsssyann_No ratings yet
- Ignou Front PageDocument1 pageIgnou Front Pageakashyadav433No ratings yet
- Notice of Thesis SubmissionDocument3 pagesNotice of Thesis Submissionmzakie66No ratings yet
- BSI UKCA Marking Enquiry Form Company Product ProfileDocument3 pagesBSI UKCA Marking Enquiry Form Company Product ProfileRizwanNo ratings yet
- 2010 03 09 Visa Form PDFDocument1 page2010 03 09 Visa Form PDFJoe HungNo ratings yet
- Lady Shri Ram College FormDocument5 pagesLady Shri Ram College Formkaidogamer686No ratings yet
- UG Student New Membership FormDocument2 pagesUG Student New Membership FormAmandi PiumikaNo ratings yet
- Mks CPSB Form 2022Document3 pagesMks CPSB Form 2022Eunice Mueni paulNo ratings yet
- Undertaking: Annexure-ADocument1 pageUndertaking: Annexure-AsurjitNo ratings yet
- Declaration Forms 2023Document2 pagesDeclaration Forms 2023hljuristsinternationalNo ratings yet
- Institute of Medical Sciences: Roll No. Banaras Hindu University VaranasiDocument8 pagesInstitute of Medical Sciences: Roll No. Banaras Hindu University Varanasianon-998406No ratings yet
- Sikkim University: Application Form (Teaching Positions)Document15 pagesSikkim University: Application Form (Teaching Positions)shantidsaNo ratings yet
- Recruitment Application Form General OCT2011Document4 pagesRecruitment Application Form General OCT2011Andre UlaanNo ratings yet
- Sastra ApplicationDocument8 pagesSastra ApplicationMaheshSrikakulamNo ratings yet
- Application Form Sac PDFDocument7 pagesApplication Form Sac PDFdasunwk4No ratings yet
- HR-104!90!20 Job Application Form For Academic PositionDocument3 pagesHR-104!90!20 Job Application Form For Academic PositionMohana SundaramNo ratings yet
- Application Form Professnal 2019Document5 pagesApplication Form Professnal 2019Jayathri PasanNo ratings yet
- Color Enquiry Form DocumentDocument4 pagesColor Enquiry Form DocumentKULDEEP PALANo ratings yet
- Sri Chaitanya Junior CollegeDocument1 pageSri Chaitanya Junior CollegeBHAVANI VISWANATHNo ratings yet
- Advisory Board Member FormDocument2 pagesAdvisory Board Member FormAna IrinaNo ratings yet
- Registration Form: Ref: Advertisement No: 37/2020-HRD Post Code No.:...............Document2 pagesRegistration Form: Ref: Advertisement No: 37/2020-HRD Post Code No.:...............ankitNo ratings yet
- Tribhuvan University: Faculty of Humanities & Social Sciences Office of The DeanDocument2 pagesTribhuvan University: Faculty of Humanities & Social Sciences Office of The DeanYouTube SubscriberNo ratings yet
- Format of Undertaking FOR CUSBDocument1 pageFormat of Undertaking FOR CUSBRajnish SinghNo ratings yet
- Application Non-Teaching2019 (F)Document3 pagesApplication Non-Teaching2019 (F)gourkanti213No ratings yet
- Sastra University: Thanjavur - 613 401, Tamil NaduDocument8 pagesSastra University: Thanjavur - 613 401, Tamil Nadue_sarath225No ratings yet
- V.B.S. Purvanchal University, Jaunpur (U.P.) - 222203: Application Form For The Teaching PostsDocument14 pagesV.B.S. Purvanchal University, Jaunpur (U.P.) - 222203: Application Form For The Teaching Postsashish7185No ratings yet
- Visa Application Form VietnamDocument2 pagesVisa Application Form Vietnam77662No ratings yet
- Enclosure IDocument1 pageEnclosure IManaf BasheerNo ratings yet
- HYA Form Silver Ilovepdf CompressedDocument1 pageHYA Form Silver Ilovepdf CompressedUtkarsh VasaniNo ratings yet
- The Forensic Documentation Sourcebook: The Complete Paperwork Resource for Forensic Mental Health PracticeFrom EverandThe Forensic Documentation Sourcebook: The Complete Paperwork Resource for Forensic Mental Health PracticeRating: 1 out of 5 stars1/5 (1)
- 0500 First Language English: MARK SCHEME For The May/June 2007 Question PaperDocument6 pages0500 First Language English: MARK SCHEME For The May/June 2007 Question PaperNizar MuhammadNo ratings yet
- List of English Extreme AdjectivesDocument2 pagesList of English Extreme AdjectivesNizar MuhammadNo ratings yet
- © This Printable Teacher Worksheet Is FromDocument2 pages© This Printable Teacher Worksheet Is FromNizar MuhammadNo ratings yet
- Extremeadj PDFDocument5 pagesExtremeadj PDFNizar MuhammadNo ratings yet
- PV1Document1 pagePV1Nizar MuhammadNo ratings yet
- အသစ္ျပဳျပင္ျပဌာန္းထားေသာ ဂ်ပန္ လူ၀င္မႈႀကီးၾကပ္ေရး ဥပေဒDocument18 pagesအသစ္ျပဳျပင္ျပဌာန္းထားေသာ ဂ်ပန္ လူ၀င္မႈႀကီးၾကပ္ေရး ဥပေဒMai Kyaw OoNo ratings yet
- Rohingya EssayDocument3 pagesRohingya EssayJohn Honder63% (8)
- Slavs in Antiquity - Valentin VDocument2 pagesSlavs in Antiquity - Valentin VJelena JovanovićNo ratings yet
- XincaDocument4 pagesXincaRobJeanNo ratings yet
- FILIPINIZATIONDocument2 pagesFILIPINIZATIONVim ApostolNo ratings yet
- Jordan VisaDocument4 pagesJordan VisaJames TeufenNo ratings yet
- Population of IndiaDocument4 pagesPopulation of IndiaGirijesh PandeyNo ratings yet
- 11 Global MigrationDocument10 pages11 Global MigrationLeah Campollo100% (2)
- Cuttack District: Orissa Review (Census Special)Document4 pagesCuttack District: Orissa Review (Census Special)Anonymous im9mMa5No ratings yet
- 06 Chapter 4 Demographic Profile and Settlement Pattern-26 July 2013Document20 pages06 Chapter 4 Demographic Profile and Settlement Pattern-26 July 2013Disha kothariNo ratings yet
- Trends in MigrationDocument10 pagesTrends in MigrationEman NolascoNo ratings yet
- International Journal of Economic Practices and TheoriesDocument14 pagesInternational Journal of Economic Practices and TheoriesElena PradaNo ratings yet
- Bangsamoro, Lumad, and Migrant SettlersDocument18 pagesBangsamoro, Lumad, and Migrant SettlersMarsgann Patrick Bartiana ParasNo ratings yet
- Bi Form Cgaf-001-Rev 2Document2 pagesBi Form Cgaf-001-Rev 2Nerissa de jesus60% (5)
- The Woman QuestionDocument40 pagesThe Woman QuestionWalid Ben MadaniNo ratings yet
- Deum03536315ma890629 PDFDocument2 pagesDeum03536315ma890629 PDFMariusCalinnNo ratings yet
- Front 23 JulyDocument1 pageFront 23 JulyRebecca BlackNo ratings yet
- 3.3 ImmigrationDocument15 pages3.3 ImmigrationIbrar ShahNo ratings yet
- Federation of Malaya: Persekutuan Tanah Melayu (PTM)Document22 pagesFederation of Malaya: Persekutuan Tanah Melayu (PTM)Cruise_IceNo ratings yet
- 6 24 13Document20 pages6 24 13The University Daily KansanNo ratings yet
- Research MethodologyDocument20 pagesResearch MethodologySahil BansalNo ratings yet
- Ethnicity Lecture 2Document21 pagesEthnicity Lecture 2api-94057686No ratings yet
- ImmigrationDocument3 pagesImmigrationapi-252808043No ratings yet
- Brides, 2004. Film Directed by Pantelis Voulgaris. Script: Joanna Karystiani. Executive Director: Martin ScorceseDocument2 pagesBrides, 2004. Film Directed by Pantelis Voulgaris. Script: Joanna Karystiani. Executive Director: Martin ScorceseHellenicNo ratings yet
- ChecklistDocument1 pageChecklistBETARTEHNo ratings yet
- PCC Application Form 270215Document2 pagesPCC Application Form 270215battlestrokerNo ratings yet
- Business Visa Requirements - NorwayDocument2 pagesBusiness Visa Requirements - Norwaygp_ph86No ratings yet
- Requesting Latvian CitizenshipDocument3 pagesRequesting Latvian CitizenshipJuliet SyNo ratings yet
- Global Demography TCWDocument17 pagesGlobal Demography TCWArold MendizabalNo ratings yet