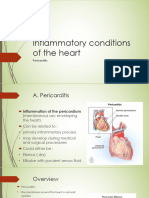
PERICARDITIS
Key signs and symptoms
Acute pericarditis
• Pericardial friction rub (grating sound heard as the heart
moves)
• Sharp and usually sudden pain that usually starts over the sternum
and radiates to the neck, shoulders, back, and arms (unlike
the pain of MI, pericardial pain is commonly pleuritic, increasing
with deep inspiration and decreasing when the client sits up and
leans forward, pulling the heart away from the diaphragmatic
pleurae of the lungs)
Chronic pericarditis
• Pericardial friction rub
• Symptoms similar to those of chronic right-sided heart failure
(fluid retention, ascites, hepatomegaly)
Key test results
• Echocardiography confirms the diagnosis when it shows an
echo-free space between the ventricular wall and the pericardium
(in cases of pleural effusion).
• ECG shows the following changes in acute pericarditis:
elevation of ST segments in the standard limb leads and most
precordial leads without significant changes in QRS morphology
that occur with MI, atrial ectopic rhythms such as atrial fibrillation,
and diminished QRS voltage in pericardial effusion.
Key treatments
• Bed rest
• Surgery: pericardiocentesis (in cases of cardiac tamponade),
partial pericardectomy (for recurrent pericarditis), total pericardectomy
(for constrictive pericarditis)
• Antibiotics: according to sensitivity of infecting organism
Key interventions
• Provide complete bed rest.
• Assess pain in relation to respiration and body position.
• Place the client in an upright position.
• Provide analgesics and oxygen, and reassure the client
with acute pericarditis that his condition is temporary and
treatable.
You might also like
- 115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p53Document1 page115-NCLEX-RN Review Made Incredibly Easy, Fifth Edition (Incredibly Easy Series) - Lippincott-16083 - p53MuhNatsirNo ratings yet
- Cardiac Tamponade & Pericardial DiseasesDocument15 pagesCardiac Tamponade & Pericardial DiseasesSamiha HassanNo ratings yet
- Cardiovascular DisordersDocument20 pagesCardiovascular DisordersHampson MalekanoNo ratings yet
- Restrictive Cardiomyopathy UtkarshDocument15 pagesRestrictive Cardiomyopathy Utkarshcrgmkps6chNo ratings yet
- Ischemic Heart Diseases: Clinical Session: Prof. Ahmed Tamara, MD Dr. Mahmoud Baraka, MDDocument28 pagesIschemic Heart Diseases: Clinical Session: Prof. Ahmed Tamara, MD Dr. Mahmoud Baraka, MDNouran AliNo ratings yet
- Chapter 4e Internal MedicineDocument19 pagesChapter 4e Internal MedicinepodmmgfNo ratings yet
- Ischemic Heart DiseaseDocument24 pagesIschemic Heart DiseaseMartha ChaseNo ratings yet
- Cardiac PathophysiologyDocument83 pagesCardiac PathophysiologyJauhar Anindita SariNo ratings yet
- Cardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarDocument23 pagesCardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarD. Melba S.S ChinnaNo ratings yet
- Valvular Heart DiseaseDocument55 pagesValvular Heart Diseaseapi-19916399No ratings yet
- Approach To Cardiovascular DiseaseDocument23 pagesApproach To Cardiovascular DiseasesanjivdasNo ratings yet
- Pericardium PDFDocument50 pagesPericardium PDFRawabi rawabi1997No ratings yet
- CARDIODocument6 pagesCARDIOEndla SriniNo ratings yet
- Chest PainDocument35 pagesChest PainSuyash SinghNo ratings yet
- Cardiac Emergency PDFDocument62 pagesCardiac Emergency PDFJose Paul RaderNo ratings yet
- Diseases of Cardiovascular SystemDocument31 pagesDiseases of Cardiovascular Systemapi-19641337No ratings yet
- AORTIC DissectionDocument20 pagesAORTIC Dissectionpaulyn ramos100% (1)
- Etiology: Clinical FeaturesDocument2 pagesEtiology: Clinical FeaturesAmalNo ratings yet
- Screening For Cardiovascular SystemDocument94 pagesScreening For Cardiovascular SystemWalijaNo ratings yet
- Cardiovascular Review II: Ana H. Corona, MSN, FNP-C Nursing Instructor October 2007Document79 pagesCardiovascular Review II: Ana H. Corona, MSN, FNP-C Nursing Instructor October 2007leesteph78No ratings yet
- Angina Pectoris 2Document47 pagesAngina Pectoris 2inyanji.barasaNo ratings yet
- Coronaryarterydisease 12866263519592 Phpapp02Document44 pagesCoronaryarterydisease 12866263519592 Phpapp02Gerome ManantanNo ratings yet
- 5+2 Chest PainDocument27 pages5+2 Chest PainMazen HossamNo ratings yet
- Acute Coronary SyndromDocument6 pagesAcute Coronary SyndromAster WidodoNo ratings yet
- Pericardial Diseases - Raghad DghaishDocument32 pagesPericardial Diseases - Raghad Dghaish180045No ratings yet
- REVISED Myocarditis Pericardititis EndocarditisDocument29 pagesREVISED Myocarditis Pericardititis EndocarditisDanial HassanNo ratings yet
- Cardiomyopathy and MyocarditisDocument8 pagesCardiomyopathy and MyocarditissarrvinrajNo ratings yet
- Cardiovascular Emergency..Document120 pagesCardiovascular Emergency..MarcellRaymondNo ratings yet
- Acute Coronary SyndromesDocument47 pagesAcute Coronary SyndromeshorosuNo ratings yet
- CVS 2Document12 pagesCVS 2duniayanNo ratings yet
- Diagnosis Gangguan KardiovaskulerDocument41 pagesDiagnosis Gangguan KardiovaskulerFifit SiePutry BintaNgnya KudaciNo ratings yet
- Curs 9 Myocarditis CardiomyopathyDocument41 pagesCurs 9 Myocarditis CardiomyopathyIliescu DenisaNo ratings yet
- An Introduction To The 12 Lead EcgDocument85 pagesAn Introduction To The 12 Lead EcgAris Diyan YulistiawanNo ratings yet
- Chest Pain Non TraumaDocument45 pagesChest Pain Non TraumaTita LuthfiaNo ratings yet
- HF & ShockDocument18 pagesHF & ShockSahar YousifNo ratings yet
- Differential Diagnosis of Cardiovascular SystemDocument50 pagesDifferential Diagnosis of Cardiovascular Systemkashmala afzalNo ratings yet
- Inflammatory Disorders PDFDocument41 pagesInflammatory Disorders PDFMoon KillerNo ratings yet
- Cardiovascular Examination 1Document43 pagesCardiovascular Examination 1ערין גבאריןNo ratings yet
- Stable Angina PectorisDocument11 pagesStable Angina Pectorismarco_bawNo ratings yet
- Pericardialdiseases 190121084846Document65 pagesPericardialdiseases 190121084846Insta GrammerNo ratings yet
- PERICARDITISDocument17 pagesPERICARDITISLydia Lopz MsnrncdNo ratings yet
- Ischemic Heart Disease. Angina Pectoris. Acute Coronary SyndromeDocument20 pagesIschemic Heart Disease. Angina Pectoris. Acute Coronary SyndromeMohammad FarizNo ratings yet
- Pathology of The Cardiovascular System-2Document24 pagesPathology of The Cardiovascular System-2AZALEA SANIANONo ratings yet
- Pericardial DX Endocarditis MyocarditisDocument74 pagesPericardial DX Endocarditis MyocarditisJefry SNo ratings yet
- Book Reading-Heart Disease Braunwald: Chapter 4 Physical Examination of The Heart and Circulation (I)Document29 pagesBook Reading-Heart Disease Braunwald: Chapter 4 Physical Examination of The Heart and Circulation (I)Jerrod WilsonNo ratings yet
- Cardio NclexDocument40 pagesCardio NclexGabrielle WashingtonNo ratings yet
- NCM 102Document9 pagesNCM 102wooooo010056100% (1)
- 4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - SurgeryDocument60 pages4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - Surgeryqobsar100% (1)
- Talley Sum UpDocument51 pagesTalley Sum UpRozana Bawareth100% (1)
- Nyeri Dada Dalam EmergensiDocument18 pagesNyeri Dada Dalam EmergensiSyukran AbNo ratings yet
- Trauma ThoraksDocument54 pagesTrauma ThoraksLisana ShidqiNo ratings yet
- Cardiovascular Clinical SkillDocument51 pagesCardiovascular Clinical SkillNadya NovianiNo ratings yet
- PericarditisDocument120 pagesPericarditisCalin Popa100% (1)
- Unstable Angina (UAP) and non-STEMIDocument66 pagesUnstable Angina (UAP) and non-STEMIIddrisu Abdul-AzizNo ratings yet
- ArrhythmiasDocument14 pagesArrhythmiasHaribabuBabuNo ratings yet
- Aortic Aneurysms: Surgical Nursing IDocument22 pagesAortic Aneurysms: Surgical Nursing ImujunisamdoNo ratings yet
- Acute Heart FailureDocument48 pagesAcute Heart FailurehorosuNo ratings yet
- Cardiac EmergenciesDocument18 pagesCardiac EmergenciesJoice DasNo ratings yet
- Cardiac Tamponade: Zhiarina Kyla M. BizDocument12 pagesCardiac Tamponade: Zhiarina Kyla M. BizMatt Joseph Cabanting100% (1)
- The Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesFrom EverandThe Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesNo ratings yet
- CIP Com Dev 2018Document4 pagesCIP Com Dev 2018choobiNo ratings yet
- Advanced Concepts in Critical Care NursingDocument3 pagesAdvanced Concepts in Critical Care Nursingchoobi100% (1)
- Impact of Simulation-Based Teaching On Nursing Pharmacology Knowledge and Clinical CompetenceDocument2 pagesImpact of Simulation-Based Teaching On Nursing Pharmacology Knowledge and Clinical CompetencechoobiNo ratings yet
- Advanced Concepts in Critical Care NursingDocument3 pagesAdvanced Concepts in Critical Care Nursingchoobi100% (1)
- ACCOMPLISHMENT REPORT On FAC. DEVDocument3 pagesACCOMPLISHMENT REPORT On FAC. DEVchoobiNo ratings yet
- Universal Prec QuestionsDocument8 pagesUniversal Prec QuestionschoobiNo ratings yet
- Nres 1 Instructional PlanDocument10 pagesNres 1 Instructional PlanchoobiNo ratings yet
- NEW BSN CURRICULUM - CMO 15 RevisedDocument2 pagesNEW BSN CURRICULUM - CMO 15 RevisedchoobiNo ratings yet
- Topics On Skills Lab Second SemDocument4 pagesTopics On Skills Lab Second SemchoobiNo ratings yet
- Assessment of Pulse SitesDocument2 pagesAssessment of Pulse SiteschoobiNo ratings yet
- Your Time Is LimitedDocument1 pageYour Time Is LimitedchoobiNo ratings yet
- level-of-disaster-preparedness-EDITED 1Document16 pageslevel-of-disaster-preparedness-EDITED 1choobiNo ratings yet
- Caselet School HealthDocument3 pagesCaselet School HealthchoobiNo ratings yet
- Nurse RoleDocument1 pageNurse RolechoobiNo ratings yet
- Quiz On School Health NursingDocument7 pagesQuiz On School Health Nursingchoobi0% (2)
- Eval Exam CHNDocument4 pagesEval Exam CHNchoobiNo ratings yet
- EVAL School Health NursingDocument4 pagesEVAL School Health NursingchoobiNo ratings yet