You might also like
- Prosthodonticsdd2011-2012 DR GhadeerDocument172 pagesProsthodonticsdd2011-2012 DR GhadeerGhadeerHassaan100% (5)
- Nasolabial Flap For Oral Cavity ReconstructionDocument10 pagesNasolabial Flap For Oral Cavity ReconstructionJamesNo ratings yet
- PV - Dark Souls 3 Guide 100%Document15 pagesPV - Dark Souls 3 Guide 100%Tepi MpeiNo ratings yet
- PAFPRS DIssection Manual (Edited)Document39 pagesPAFPRS DIssection Manual (Edited)Aileen Delos Santos-Garcia100% (2)
- 2010 Facial Degloving Approach To The MidfaceDocument4 pages2010 Facial Degloving Approach To The MidfaceAFJimenezONo ratings yet
- IPE Beams Dimensions and PropertiesDocument2 pagesIPE Beams Dimensions and PropertiesGalih Santana0% (1)
- Use of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFDocument9 pagesUse of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFJose Luis Granados SolerNo ratings yet
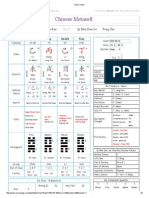
- Ba Zi Chart1Document2 pagesBa Zi Chart1adisebe100% (1)
- 13 Neutral ZoneDocument3 pages13 Neutral Zonedrgayen6042No ratings yet
- Pakistan Studies Complete Notes (Question Answer Format)Document215 pagesPakistan Studies Complete Notes (Question Answer Format)Hafiz Ashfaq Ahmed91% (530)
- Surgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDocument4 pagesSurgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDwarika Prasad BajgaiNo ratings yet
- B-63874en-1 - 08 Manual Guide I Set-Up Guidance FunctionsDocument328 pagesB-63874en-1 - 08 Manual Guide I Set-Up Guidance FunctionsGiang Nguyen VanNo ratings yet
- Ahead 29 NTH Dec Online Live Lecture MCQDocument50 pagesAhead 29 NTH Dec Online Live Lecture MCQAhead Dental Coaching100% (1)
- Informatica TutorialsDocument2 pagesInformatica Tutorialsj_jeevan_jNo ratings yet
- Recontruccion LabialDocument23 pagesRecontruccion LabialJezreel Ortiz AscenciónNo ratings yet
- 10 16 02CleftLipandPalatePart2 PDFDocument93 pages10 16 02CleftLipandPalatePart2 PDFalinutza_childNo ratings yet
- Lip Reconstruction: Learning ObjectivesDocument8 pagesLip Reconstruction: Learning Objectivesalinutza_childNo ratings yet
- Verschueren Jef.-Understanding PragmaticsDocument309 pagesVerschueren Jef.-Understanding PragmaticsMahfoodh AljubouryNo ratings yet
- A Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryDocument9 pagesA Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryJWPlasticsurgeryNo ratings yet
- IB Biology Lab Report GuideDocument16 pagesIB Biology Lab Report Guideaufafua100% (1)
- Irving FisherDocument26 pagesIrving FisherWilson SequeiraNo ratings yet
- 10-16-02 Cleft Lip and Palate Part 2 TEKNIKDocument93 pages10-16-02 Cleft Lip and Palate Part 2 TEKNIKSulistyawati WrimunNo ratings yet
- The Use of A Cutaneous Muscular Flap For Primary Naso Labial Repair With A Modified Tennison Randal TechniqueDocument4 pagesThe Use of A Cutaneous Muscular Flap For Primary Naso Labial Repair With A Modified Tennison Randal TechniqueShaly MaduroNo ratings yet
- MandibulectomiaDocument8 pagesMandibulectomiaCarlos Eduardo BordaNo ratings yet
- Head and Neck Cancer - Reconstruction: HistoryDocument6 pagesHead and Neck Cancer - Reconstruction: HistorySri MahyantiNo ratings yet
- Bilateral Cleft Lip ReconstructionDocument14 pagesBilateral Cleft Lip ReconstructionHusni mubarakNo ratings yet
- Amalgam Carving TechniqueDocument5 pagesAmalgam Carving Techniquearun3883No ratings yet
- Repair of A Large Defect of The Upper LipDocument4 pagesRepair of A Large Defect of The Upper LipdoctorbanNo ratings yet
- Secondary Deofrmities of Cleft Lip NoseDocument8 pagesSecondary Deofrmities of Cleft Lip NoseahmedatefNo ratings yet
- 5657 DownDocument17 pages5657 DownMai ThúyNo ratings yet
- 38 Lip Reconstruction: Babak J.Mehrara, M.D., and Barry M.Zide, M.D., D.M.DDocument15 pages38 Lip Reconstruction: Babak J.Mehrara, M.D., and Barry M.Zide, M.D., D.M.Dandre andreNo ratings yet
- Caloss2013 PDFDocument221 pagesCaloss2013 PDFsriwahyuutamiNo ratings yet
- Modified FAMMDocument4 pagesModified FAMMSilverline TeamNo ratings yet
- Description of Nasoalveolar Molding Process in Neonatal Period of Unilateral Cleft Lip and Palate: A Step by StepDocument5 pagesDescription of Nasoalveolar Molding Process in Neonatal Period of Unilateral Cleft Lip and Palate: A Step by StepwijdaneNo ratings yet
- 2007 O To Z Reconstruction of Central Upper Lip DefectDocument5 pages2007 O To Z Reconstruction of Central Upper Lip DefectDimitris RodriguezNo ratings yet
- Primary Cleft Lip and Palate Amit PapnejaDocument5 pagesPrimary Cleft Lip and Palate Amit PapnejaAmit PapnejaNo ratings yet
- Bilateral Cleft Lip and Whistling Deformity The X.43Document6 pagesBilateral Cleft Lip and Whistling Deformity The X.43rupak979No ratings yet
- Ideas and Innovations: George L. Murrell, M.D., Ricardo Requena, D.O., and Daniel W. Karakla, M.DDocument5 pagesIdeas and Innovations: George L. Murrell, M.D., Ricardo Requena, D.O., and Daniel W. Karakla, M.DVijay Prabu GNo ratings yet
- Primary Correction of The Unilateral Cleft Lip Nasal Deformity: Achieving The ExcellenceDocument6 pagesPrimary Correction of The Unilateral Cleft Lip Nasal Deformity: Achieving The ExcellenceDesrainy InhardiniNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Nanda Anggita P PNo ratings yet
- One Stage Aesthetic and Functional Reconstruction of Major Lower Lip DefectsDocument5 pagesOne Stage Aesthetic and Functional Reconstruction of Major Lower Lip DefectsDr. Hilder HernandezNo ratings yet
- Simultaneous Reconstruction of The Secondary Bilateral Cleft Lip and Nasal Deformity: Abbé Flap RevisitedDocument9 pagesSimultaneous Reconstruction of The Secondary Bilateral Cleft Lip and Nasal Deformity: Abbé Flap RevisitedwulanbrurrNo ratings yet
- The Bozola Flap in Oral Cavity Reconstruction PDFDocument4 pagesThe Bozola Flap in Oral Cavity Reconstruction PDFPorcupine TreeNo ratings yet
- SulcoplastyDocument2 pagesSulcoplastyInayatul MaulanaNo ratings yet
- Modified Pontic Design For Ridge DefectsDocument11 pagesModified Pontic Design For Ridge DefectsFaheemuddin MuhammadNo ratings yet
- Primary RhinoplastyDocument7 pagesPrimary Rhinoplastysmansa123No ratings yet
- Secondary Rhinoplastyin Unilateralcleft Nasaldeformity: Tom D. WangDocument5 pagesSecondary Rhinoplastyin Unilateralcleft Nasaldeformity: Tom D. WangSiska HarapanNo ratings yet
- Manejo Dentofacial Del Paciente Con Labio y Paladar HendidoDocument8 pagesManejo Dentofacial Del Paciente Con Labio y Paladar HendidoGilberto Aaron Osorio PiaNo ratings yet
- Shetye 2017Document7 pagesShetye 2017Evgeniya KocherginaNo ratings yet
- Aesthetic Lip SplitsDocument4 pagesAesthetic Lip Splitsrajtanniru100% (1)
- Gomez Et Al 2012Document12 pagesGomez Et Al 2012LAURA MARCELA BARRENECHE CALLENo ratings yet
- The Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North AmerDocument9 pagesThe Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North Amerlaljadeff12No ratings yet
- Suture TipDocument5 pagesSuture Tipstéphan AlessandroNo ratings yet
- Management of The Mucolabial Fold When Developing Impressions For Complete DenturesDocument6 pagesManagement of The Mucolabial Fold When Developing Impressions For Complete Denturesjinny1_0No ratings yet
- Reconstruction of Intraoral Defects Using Facial Artery Musculomucosal FlapDocument6 pagesReconstruction of Intraoral Defects Using Facial Artery Musculomucosal FlapRajan KarmakarNo ratings yet
- Cleft Lip & Palate SurgeryDocument5 pagesCleft Lip & Palate SurgeryShoaib A. KaziNo ratings yet
- Tongue FlapDocument12 pagesTongue Flap6hd6mnrzw2No ratings yet
- Review Article: Barry H. Grayson, Pradip R. ShetyeDocument7 pagesReview Article: Barry H. Grayson, Pradip R. ShetyeHARITHA H.PNo ratings yet
- Lip Reconstruction: Donald Baumann, M.D., and Geoffrey Robb, M.DDocument12 pagesLip Reconstruction: Donald Baumann, M.D., and Geoffrey Robb, M.DBenedetta GuarinoNo ratings yet
- A Classification System of DefectsDocument12 pagesA Classification System of DefectsPrana SkyaNo ratings yet
- Subperiosteal Chin Augmentation With Hyaluronic AcDocument10 pagesSubperiosteal Chin Augmentation With Hyaluronic AcPriscilla SamuelNo ratings yet
- Monobloc and Facial Bipartition OsteotomiesDocument18 pagesMonobloc and Facial Bipartition OsteotomiesKim SalahNo ratings yet
- A Hollow Delayed Surgical ObturatorDocument55 pagesA Hollow Delayed Surgical ObturatorvinnycoolbuddyNo ratings yet
- Article-PDF-sandeep Garg Sushant Garg Mohit Mehta Sangeeta Goyal-286Document3 pagesArticle-PDF-sandeep Garg Sushant Garg Mohit Mehta Sangeeta Goyal-286Mrunal DoiphodeNo ratings yet
- Fabrication of Conventional Complete Dentures For A Left Segmental MandibulectomyDocument4 pagesFabrication of Conventional Complete Dentures For A Left Segmental MandibulectomyIndrani DasNo ratings yet
- Klein 1984Document6 pagesKlein 1984Diana ZamalloaNo ratings yet
- Ovate PDFDocument11 pagesOvate PDFAriPratiwiNo ratings yet
- The Family Man S02E04 Eagle 1080p Amzn WEBcDocument50 pagesThe Family Man S02E04 Eagle 1080p Amzn WEBcAbhinav JhadeNo ratings yet
- HSO408 Assessment 2 Expanded Rubrics - FINAL2019Document5 pagesHSO408 Assessment 2 Expanded Rubrics - FINAL2019sidney drecotteNo ratings yet
- Bece English TestDocument2 pagesBece English TestASARENo ratings yet
- Speaking Tips For IELTS EXAMDocument17 pagesSpeaking Tips For IELTS EXAMBe ForqNo ratings yet
- Development of A Reliability Based Design Framework For Transmission Line Structure FoundationsDocument9 pagesDevelopment of A Reliability Based Design Framework For Transmission Line Structure FoundationsNitesh JainNo ratings yet
- Influence of Korean DramaDocument19 pagesInfluence of Korean DramaFlorie Jane Prado BagaanNo ratings yet
- The Moon: The Moon Abiding in The Midst of Serene Mind Great Waves Breaking Into LightDocument3 pagesThe Moon: The Moon Abiding in The Midst of Serene Mind Great Waves Breaking Into LightmetaltigerNo ratings yet
- Week 4Document12 pagesWeek 4Norhidayah RahmanNo ratings yet
- Lecture Notes On Mathematical Olympiad Courses: For Junior Section Vol. 2Document12 pagesLecture Notes On Mathematical Olympiad Courses: For Junior Section Vol. 2cheintNo ratings yet
- Post Colonial LiteratureDocument16 pagesPost Colonial LiteratureVivi Lujan GarellisNo ratings yet
- IctfpdDocument2 pagesIctfpdapi-409798698No ratings yet
- Presented By-: Dr. Prabhata Kumar Parida ADM - No. 06ARGO/13Document19 pagesPresented By-: Dr. Prabhata Kumar Parida ADM - No. 06ARGO/13Krushna krupa PradhanNo ratings yet
- Erp Testing PDFDocument2 pagesErp Testing PDFChelseaNo ratings yet
- 38 Pamintuan v. CADocument1 page38 Pamintuan v. CAJoshua Alexander CalaguasNo ratings yet
- ADMU V CapulongDocument21 pagesADMU V CapulongjunjunNo ratings yet
- Goldman Sachs - Internal Audit - Model RiskDocument2 pagesGoldman Sachs - Internal Audit - Model Riskadityaacharya44No ratings yet
- The Atlantic Monthly, Volume 12, No. 69, July, 1863 by VariousDocument145 pagesThe Atlantic Monthly, Volume 12, No. 69, July, 1863 by VariousGutenberg.orgNo ratings yet
- The Solitary ReaperDocument2 pagesThe Solitary ReaperTaibur RahamanNo ratings yet
- 3 Affect Regulation, Mentalization, and The Development of The Self (Peter Fonagy, Gyorgy Gergely, Elliot L. Jurist Etc.) - 211-259Document49 pages3 Affect Regulation, Mentalization, and The Development of The Self (Peter Fonagy, Gyorgy Gergely, Elliot L. Jurist Etc.) - 211-259Sergio Andres Rico AvendanoNo ratings yet
- PersonalityDocument3 pagesPersonalityManjae CamielaNo ratings yet
- Resume (Ritz) - CSRDocument3 pagesResume (Ritz) - CSRAngelie MadrigalNo ratings yet