You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 1-Frcem Primary Recalls-EXAM COLLECTIONDocument18 pages1-Frcem Primary Recalls-EXAM COLLECTIONHossamNo ratings yet
- Joe Iwanaga, R. Shane Tubbs - Atlas of Oral and Maxillofacial Anatomy-Springer (2021)Document170 pagesJoe Iwanaga, R. Shane Tubbs - Atlas of Oral and Maxillofacial Anatomy-Springer (2021)duymerNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
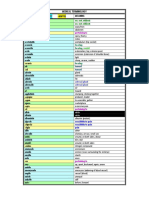
- Medical Term List PDFDocument21 pagesMedical Term List PDFAntonSusantoNo ratings yet
- Physics Project On Total Internal ReflectionDocument20 pagesPhysics Project On Total Internal ReflectionDivyanshu Gupta61% (18)
- Semiconductor Thermogenerator: by Divyanshu Gupta 2015B5A80515GDocument10 pagesSemiconductor Thermogenerator: by Divyanshu Gupta 2015B5A80515GDivyanshu GuptaNo ratings yet
- Zeeman Effect: 1 Aim of The ExperimentDocument1 pageZeeman Effect: 1 Aim of The ExperimentDivyanshu GuptaNo ratings yet
- Chemistry Investigatory ProjectDocument21 pagesChemistry Investigatory ProjectDivyanshu Gupta33% (3)
- Word Power Made Easy PDFDocument272 pagesWord Power Made Easy PDFNgaonii Panii Pou0% (3)
- MathsDocument15 pagesMathsDivyanshu GuptaNo ratings yet
- Soccer Unit Plan: Erin Railing Arin YarcDocument38 pagesSoccer Unit Plan: Erin Railing Arin YarcDivyanshu GuptaNo ratings yet
- (Ed Mir) Irodov - Problems in General Physics (Eng)Document197 pages(Ed Mir) Irodov - Problems in General Physics (Eng)Divyanshu Gupta100% (1)
- When I Stood For My Classmate!: Based On A Story Set in The 7940sDocument35 pagesWhen I Stood For My Classmate!: Based On A Story Set in The 7940scariappakc100% (2)
- At The Beginning of The New MillenniumDocument2 pagesAt The Beginning of The New MillenniumDivyanshu GuptaNo ratings yet
- Ans. Xanthelasma Answer Peripheral CyanosisDocument2 pagesAns. Xanthelasma Answer Peripheral CyanosisJordan Abosama MamalumpongNo ratings yet
- 9.1 Plant Structure and Growth: Topic 9: Plant Science (HL)Document6 pages9.1 Plant Structure and Growth: Topic 9: Plant Science (HL)Morgan LockeNo ratings yet
- HA FinalDocument209 pagesHA Finalclaire3230No ratings yet
- OrchiectomyDocument28 pagesOrchiectomytutorial 18No ratings yet
- Information Processing TheoryDocument43 pagesInformation Processing TheoryALISH AGRAWALNo ratings yet
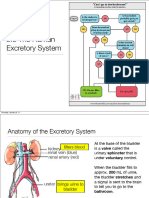
- SBI4U Unit 4 Homeostasis Excretory SystemDocument27 pagesSBI4U Unit 4 Homeostasis Excretory System전채연No ratings yet
- Antihypertensive Drugs - Classification & MechanismDocument1 pageAntihypertensive Drugs - Classification & MechanismAhmed YT100% (1)
- Drug Study LRDRDocument6 pagesDrug Study LRDRMeagan Gail Savella GarciaNo ratings yet
- Fever in Infants and ChildrenDocument24 pagesFever in Infants and ChildrenakbianchessiNo ratings yet
- Chest Tube Manual Atrium Green HandbookDocument40 pagesChest Tube Manual Atrium Green HandbookprogramgrabberNo ratings yet
- Genome Lab Fragment Analysis Protocol 608113Document2 pagesGenome Lab Fragment Analysis Protocol 608113Sukma AditiarNo ratings yet
- Circulatory System: Biology Chapter 6 Term 1 ST 1Document27 pagesCirculatory System: Biology Chapter 6 Term 1 ST 1Pranati SharmaNo ratings yet
- Enls V 4 0 Protocol Avs FinalDocument14 pagesEnls V 4 0 Protocol Avs Finalsucipto suciptoNo ratings yet
- InPractice2002 Martin ECGs3 PDFDocument12 pagesInPractice2002 Martin ECGs3 PDFNag Mallesh RaoNo ratings yet
- Furman 2013 Vestibular MigraineDocument10 pagesFurman 2013 Vestibular MigraineJuan Hernández GarcíaNo ratings yet
- Agung Satria Radisu I11107046Document53 pagesAgung Satria Radisu I11107046Resti Puteri ApriyuslimNo ratings yet
- June 2013 NewsletterDocument20 pagesJune 2013 Newsletterapi-129967289No ratings yet
- 2022 Masingue P.Latour Rev Neurol Genetic Analysis in HereditaryDocument20 pages2022 Masingue P.Latour Rev Neurol Genetic Analysis in HereditaryLéo VidoniNo ratings yet
- Worksheet 7 Endocrine Digestive Urinary Repro Eehhh Final PDFDocument31 pagesWorksheet 7 Endocrine Digestive Urinary Repro Eehhh Final PDFkaejane gonzagaNo ratings yet
- Act05 Animal Histology and Organology ExerciseDocument9 pagesAct05 Animal Histology and Organology ExerciseMicah Elline LontocNo ratings yet
- Ancient Science of Death and RebirthDocument258 pagesAncient Science of Death and RebirthAnonymous100% (1)
- Pharmacology For Oral RecitDocument16 pagesPharmacology For Oral RecitAngel DiangNo ratings yet
- DNA Extraction (Using The Omega Biotek E.Z.N.A. Mollusc DNA Kit)Document3 pagesDNA Extraction (Using The Omega Biotek E.Z.N.A. Mollusc DNA Kit)xicoalexandreNo ratings yet
- Medical Certificate FormatDocument1 pageMedical Certificate FormatrashmarsvNo ratings yet
- 8 Physio OB - Physiology of Labor I - IIDocument14 pages8 Physio OB - Physiology of Labor I - IIArnoldBorromeoNo ratings yet
- Gross Anatomy and Physiology of The Larynx: Samantha Soriano-Castañeda, MD, Fpso-Hns 10/30/2017Document4 pagesGross Anatomy and Physiology of The Larynx: Samantha Soriano-Castañeda, MD, Fpso-Hns 10/30/2017Abi SulitNo ratings yet
- BI550 2012 Lec02 HANDOUTDocument22 pagesBI550 2012 Lec02 HANDOUTJoycee Jatulan-EnajeNo ratings yet