You might also like
- Cardiovascular DiseasesDocument155 pagesCardiovascular DiseasesAnonymous jpBmlxOZVwNo ratings yet
- Herbal Medicine Guide to Benefits, Uses & Side EffectsDocument58 pagesHerbal Medicine Guide to Benefits, Uses & Side EffectsPrabhu Venugopal67% (3)
- DOH Manual of Operations-PhilPENDocument60 pagesDOH Manual of Operations-PhilPENKarlo Quezon100% (2)
- ASD Diagnosis Tools - UpToDateDocument3 pagesASD Diagnosis Tools - UpToDateEvy Alvionita Yurna100% (1)
- Philippine Package Essential NCD Interventions Manual of Operations 5 AprilDocument60 pagesPhilippine Package Essential NCD Interventions Manual of Operations 5 AprilCecilia Acuin67% (3)
- Manual On The PEN Protocol On The Integrated Management of Hypertension and DiabetesDocument61 pagesManual On The PEN Protocol On The Integrated Management of Hypertension and DiabetesRanda Noray100% (2)
- Medical Device Classification GuideDocument30 pagesMedical Device Classification GuideAriska Oktavera 26No ratings yet
- Restricted Drugs and Non FormularyDocument2 pagesRestricted Drugs and Non FormularyChristine Joy De OcampoNo ratings yet
- FGDP X-Ray Book Web v2 PDFDocument190 pagesFGDP X-Ray Book Web v2 PDFMariana IdorașiNo ratings yet
- MRCOG Part 2 500 SBAs and EMQs, 2nd EditionDocument335 pagesMRCOG Part 2 500 SBAs and EMQs, 2nd Editionobgyn hebatNo ratings yet
- Introduction To Community MedicineDocument6 pagesIntroduction To Community MedicineHannan Ali50% (2)
- Introduction To Community MedicineDocument6 pagesIntroduction To Community MedicineHannan Ali50% (2)
- 26a. Post Partum HemorrhageDocument35 pages26a. Post Partum HemorrhageAubrey100% (1)
- Low Gi Food ListDocument5 pagesLow Gi Food ListMhareesa BrownNo ratings yet
- Common ColdDocument6 pagesCommon ColdChastin Perias0% (1)
- Physical Education and Health 2: IN Grade 11 Quarter 4, Module 5Document9 pagesPhysical Education and Health 2: IN Grade 11 Quarter 4, Module 5triicciaa faithNo ratings yet
- The Problem and Its BackgroundDocument46 pagesThe Problem and Its Backgroundharoldpaulo100% (1)
- Noncommunicable - or Chronic - Diseases Are Diseases of Long Duration and Generally Slow ProgressionDocument3 pagesNoncommunicable - or Chronic - Diseases Are Diseases of Long Duration and Generally Slow ProgressionklaireNo ratings yet
- NCDs 2Document100 pagesNCDs 2Fauziyah Farah RNo ratings yet
- Christ The KingDocument6 pagesChrist The KingAnonymous LPp1PuzFPQNo ratings yet
- Non Communicable Diseases: Frequently Asked Questions OnDocument5 pagesNon Communicable Diseases: Frequently Asked Questions OnAnaiyur CorporationNo ratings yet
- Major Risk Factors for Cardiovascular DiseasesDocument28 pagesMajor Risk Factors for Cardiovascular DiseasesMannat ZaidiNo ratings yet
- WEEK 9 - Environmental Health and ToxicologyDocument81 pagesWEEK 9 - Environmental Health and ToxicologyRechelle Anne RondaelNo ratings yet
- Chronic DiseaseDocument6 pagesChronic DiseasekksNo ratings yet
- CancerlifestyleDocument9 pagesCancerlifestyleGia BảoNo ratings yet
- Control of Non Communicable DiseaseDocument16 pagesControl of Non Communicable DiseaseBangis YauriNo ratings yet
- Balakumar 2016Document45 pagesBalakumar 2016masNo ratings yet
- Prevent Chronic Disease with Lifestyle ChangesThis title summarizes the key message of the document by focusing on prevention of chronic diseases through lifestyle changesDocument57 pagesPrevent Chronic Disease with Lifestyle ChangesThis title summarizes the key message of the document by focusing on prevention of chronic diseases through lifestyle changesLaron BurrowsNo ratings yet
- NCDsDocument8 pagesNCDsshivani.priyaNo ratings yet
- Science and Technology Writing)Document3 pagesScience and Technology Writing)Catherine Casabuena MercadoNo ratings yet
- Report in MAPEHDocument2 pagesReport in MAPEHDavid Con RiveroNo ratings yet
- Key Facts: People at Risk of NcdsDocument4 pagesKey Facts: People at Risk of NcdsJonalyn MontecalvoNo ratings yet
- Metabolic Syndrome Diseases: Causes, Risk Factors, and Nutrition TreatmentDocument8 pagesMetabolic Syndrome Diseases: Causes, Risk Factors, and Nutrition TreatmentMahmoud SelimNo ratings yet
- M2 Non-Communicable DiseasesDocument66 pagesM2 Non-Communicable DiseasesArdra SabuNo ratings yet
- IntroductionDocument3 pagesIntroductionLIEZL NabutilNo ratings yet
- Introduction To Non-Communicable DiseasesDocument7 pagesIntroduction To Non-Communicable DiseasesSalem Nissi MayorNo ratings yet
- Noncommunicable Diseases: Dr. Muhammad Bimo Harmaji Avimsa Hima PSPD FK Unlam Januari, 2017Document33 pagesNoncommunicable Diseases: Dr. Muhammad Bimo Harmaji Avimsa Hima PSPD FK Unlam Januari, 2017dewifebrianaNo ratings yet
- CVD Effects of ExerciseDocument11 pagesCVD Effects of ExerciseAboobacker SabithNo ratings yet
- PBH 101-10 (NDS)Document14 pagesPBH 101-10 (NDS)ish ishokNo ratings yet
- Role of Personal Hygiene in Non Communicable DiseasesDocument17 pagesRole of Personal Hygiene in Non Communicable DiseasesTalal AwanNo ratings yet
- Tutorial Project NAME: Chriatiane BaronaDocument2 pagesTutorial Project NAME: Chriatiane BaronaJohn Domínguez MedinaNo ratings yet
- Case Study CVDDocument8 pagesCase Study CVDChloe AguiNo ratings yet
- ArticlesDocument955 pagesArticlesMuhammad ChohanNo ratings yet
- Lifestyle Related DiseasesDocument8 pagesLifestyle Related DiseasesEJMS1122No ratings yet
- C2 Health BenefitDocument10 pagesC2 Health BenefitHanan FuadNo ratings yet
- Unit Two The Health Benefits of Physical ActivityDocument10 pagesUnit Two The Health Benefits of Physical ActivityYoseph DefaruNo ratings yet
- Higher Risks of Cancer, Type 2 Diabetes, High Blood Pressure, Respiratory Disorders, and Cardiovascular DiseaseDocument5 pagesHigher Risks of Cancer, Type 2 Diabetes, High Blood Pressure, Respiratory Disorders, and Cardiovascular DiseaseJuveria nsNo ratings yet
- 4.prevention & ControlDocument47 pages4.prevention & Controla lu100% (1)
- Cancer, Also Known As ADocument4 pagesCancer, Also Known As AMarc Lorenz DucusinNo ratings yet
- Frontiers Management and Prevention Strategies For Non-Communicable Diseases (NCDS) and Their Risk FactorsDocument1 pageFrontiers Management and Prevention Strategies For Non-Communicable Diseases (NCDS) and Their Risk FactorsKassandra Gweneth HuganasNo ratings yet
- 261 Practice of Adults On Prevention of Hypertension and Associated Factors in Dessie Administrative City, Ethiopia, 2016Document12 pages261 Practice of Adults On Prevention of Hypertension and Associated Factors in Dessie Administrative City, Ethiopia, 2016Vibhor Kumar JainNo ratings yet
- Unit Two: 2. The Health Benefits of Physical ActivityDocument24 pagesUnit Two: 2. The Health Benefits of Physical Activityeyob astatkeNo ratings yet
- Table 1. Top Mortality in Malaysia (Source: Sa Et Al, 2013)Document4 pagesTable 1. Top Mortality in Malaysia (Source: Sa Et Al, 2013)Yusi f-vNo ratings yet
- Epidemiologi (3) : (Epidemiologi Penyakit Tidak Menular)Document10 pagesEpidemiologi (3) : (Epidemiologi Penyakit Tidak Menular)Daw AddawNo ratings yet
- Cardiologist Prof Rishi Sethi' Presentation On World Heart DayDocument36 pagesCardiologist Prof Rishi Sethi' Presentation On World Heart DaybobbyramakantNo ratings yet
- A Seminar PaperDocument14 pagesA Seminar PaperOmolosoNo ratings yet
- Lifestyle DiseasesDocument14 pagesLifestyle DiseasesMark KinotiNo ratings yet
- Osomatha OmoDocument21 pagesOsomatha OmoRichard PaulNo ratings yet
- Geriatric Aging Background Information: Chernoff, 2006Document2 pagesGeriatric Aging Background Information: Chernoff, 2006Reine SalamounNo ratings yet
- Discover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingFrom EverandDiscover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingNo ratings yet
- Day 2 - NCD - NonCOmmunicable DiseasesDocument98 pagesDay 2 - NCD - NonCOmmunicable DiseasesMary Paula EstiveNo ratings yet
- National Healthy Lifestyle ProgramDocument5 pagesNational Healthy Lifestyle ProgramShan NehNo ratings yet
- A Discussion On Main Causes and Preventive Measures of Non Communicable Diseases in RajasthanDocument22 pagesA Discussion On Main Causes and Preventive Measures of Non Communicable Diseases in RajasthanDINESHNo ratings yet
- Saklayen, M. G. (2018) - The Global Epidemic of The Metabolic Syndrome.Document8 pagesSaklayen, M. G. (2018) - The Global Epidemic of The Metabolic Syndrome.ken macNo ratings yet
- Couse of Death: 1. Poor Country 2. Developing Country 3. Developed CountryDocument13 pagesCouse of Death: 1. Poor Country 2. Developing Country 3. Developed CountryHana Fauziyah KhairunnisaNo ratings yet
- Non-Communicable Disease Prevention and Control: Jennifer S. Cruel, RN, MNDocument65 pagesNon-Communicable Disease Prevention and Control: Jennifer S. Cruel, RN, MNChoi D. CruelNo ratings yet
- Reference Material II 18Document50 pagesReference Material II 18Maru Mengesha Worku 18BBT0285100% (1)
- CVDDocument25 pagesCVDSameer ValsangkarNo ratings yet
- Maladie Chronique 2 - 113904Document11 pagesMaladie Chronique 2 - 113904Danielle MadeNo ratings yet
- Subject Psychology: Paper No.10: Psycho-Geriatrics MODULE No. 14: Hypertension and DiabetesDocument10 pagesSubject Psychology: Paper No.10: Psycho-Geriatrics MODULE No. 14: Hypertension and DiabetesManisha VarsaniNo ratings yet
- PBH 9-16Document55 pagesPBH 9-16Emran HossainNo ratings yet
- Overview of Major Noncommunicable Diseases (NCD)Document49 pagesOverview of Major Noncommunicable Diseases (NCD)Jam Knows RightNo ratings yet
- Comprehension 3 Exam #2Document3 pagesComprehension 3 Exam #2Hannan AliNo ratings yet
- State of Libya Open University 1st Semester Course ScheduleDocument5 pagesState of Libya Open University 1st Semester Course ScheduleHannan AliNo ratings yet
- Read Me PCDocument2 pagesRead Me PCKogree Kyaw Win OoNo ratings yet
- K (Document106 pagesK (Hannan AliNo ratings yet
- DM 4th Yr Student Copy 4Document1 pageDM 4th Yr Student Copy 4Hannan AliNo ratings yet
- Comprehension 3 Exam #1Document2 pagesComprehension 3 Exam #1Hannan AliNo ratings yet
- DM 4th Yr Student Copy 4Document40 pagesDM 4th Yr Student Copy 4Hannan AliNo ratings yet
- State of Libya Open University 1st Semester Course ScheduleDocument5 pagesState of Libya Open University 1st Semester Course ScheduleHannan AliNo ratings yet
- Discursive Essay GuideDocument6 pagesDiscursive Essay GuideHannan Ali67% (3)
- Composition 4 ExamDocument3 pagesComposition 4 ExamHannan AliNo ratings yet
- Composition 3 ExamDocument2 pagesComposition 3 ExamHannan AliNo ratings yet
- Composition 2 ExamDocument3 pagesComposition 2 ExamHannan AliNo ratings yet
- Basics of Nursing ScienceDocument3 pagesBasics of Nursing ScienceHannan AliNo ratings yet
- Ecology and EcosystemDocument12 pagesEcology and EcosystemHannan AliNo ratings yet
- Monthly Quiz 1Document1 pageMonthly Quiz 1Hannan AliNo ratings yet
- Custom Essay Writings: Check These Useful Tips For Writing An Opinion EssayDocument4 pagesCustom Essay Writings: Check These Useful Tips For Writing An Opinion EssayHannan AliNo ratings yet
- Epid - Xercise 2015Document1 pageEpid - Xercise 2015Hannan AliNo ratings yet
- CHRONIC NON-COMMUNICABLE DISEASES: A GLOBAL CHALLENGEDocument27 pagesCHRONIC NON-COMMUNICABLE DISEASES: A GLOBAL CHALLENGEHannan AliNo ratings yet
- Teaching PicturesDocument24 pagesTeaching PicturesHannan AliNo ratings yet
- WHO Refrigerator Guidelines For Safe Storage in The Vaccination Centers PDFDocument1 pageWHO Refrigerator Guidelines For Safe Storage in The Vaccination Centers PDFHannan AliNo ratings yet
- CHRONIC NON-COMMUNICABLE DISEASES: A GLOBAL CHALLENGEDocument27 pagesCHRONIC NON-COMMUNICABLE DISEASES: A GLOBAL CHALLENGEHannan AliNo ratings yet
- Introduction To Community MedicineDocument34 pagesIntroduction To Community MedicineHannan AliNo ratings yet
- Expermintal EpidDocument9 pagesExpermintal EpidHannan AliNo ratings yet
- Analytical StudiesDocument16 pagesAnalytical StudiesHannan AliNo ratings yet
- Epidemiology Exercises: Birth, Death, Morbidity RatesDocument1 pageEpidemiology Exercises: Birth, Death, Morbidity RatesHannan AliNo ratings yet
- Association and Cauasation LailaDocument25 pagesAssociation and Cauasation LailaHannan AliNo ratings yet
- File2-Diseases Concept 2014Document40 pagesFile2-Diseases Concept 2014Hannan AliNo ratings yet
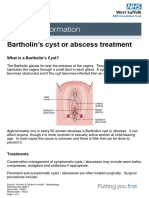
- Bartholin's Cyst or Abscess TreatmentDocument4 pagesBartholin's Cyst or Abscess TreatmentRezaFArthaNo ratings yet
- Psoriatic Arthritis Nature ReviewDocument17 pagesPsoriatic Arthritis Nature ReviewJose Shaid Delgado OlveraNo ratings yet
- NursDocument4 pagesNursapi-323159742No ratings yet
- Factors Associated With Intention To Report Child Abuse QuestionnaireDocument2 pagesFactors Associated With Intention To Report Child Abuse QuestionnaireAYESSA ALYZA MACMODNo ratings yet
- Umj7603 122Document2 pagesUmj7603 122Ifrah YousafNo ratings yet
- CV Europass CaprosDocument3 pagesCV Europass CaprosCristinaCaprosNo ratings yet
- NCCNTB Breast-Cancer 06.29.20 2up-1Document41 pagesNCCNTB Breast-Cancer 06.29.20 2up-1dianaNo ratings yet
- Infection Control and Related Health and Safety in The Dental OfficeDocument48 pagesInfection Control and Related Health and Safety in The Dental OfficeKim Lien TrinhNo ratings yet
- Liquen Plano OralDocument44 pagesLiquen Plano OralJoana MartinsNo ratings yet
- Viva XT Brochure - 201203539IEp3Document6 pagesViva XT Brochure - 201203539IEp3Lubna LuaiNo ratings yet
- Anabolic Steroids HandoutDocument4 pagesAnabolic Steroids HandoutDiana AstriaNo ratings yet
- Patient Decision Aid PDF 243780159 PDFDocument23 pagesPatient Decision Aid PDF 243780159 PDFJimboNo ratings yet
- His 5Document167 pagesHis 5Anjum100% (5)
- PRC Case Form Cmo 14Document5 pagesPRC Case Form Cmo 14iamELHIZANo ratings yet
- BMS291 Practice ExamDocument26 pagesBMS291 Practice Examsopheeyuh100% (1)
- Overview of HIV Infection & PreventionDocument29 pagesOverview of HIV Infection & PreventionNiccolo G. ChiongbianNo ratings yet
- The Developing Occlusion ofDocument6 pagesThe Developing Occlusion ofAlistair KohNo ratings yet
- Polymyalgia Rheumatica Diagnosis and TreatmentDocument7 pagesPolymyalgia Rheumatica Diagnosis and Treatmenttika tikaNo ratings yet
- Western Mindanao State UniversityDocument10 pagesWestern Mindanao State Universitynot your medz duranNo ratings yet
- Oxytocin Is Not Associated With Postpartum Hemorrhage in Labor Augmentation in A Retrospective Cohort Study in The United StatesDocument9 pagesOxytocin Is Not Associated With Postpartum Hemorrhage in Labor Augmentation in A Retrospective Cohort Study in The United Statesstat madeeasyNo ratings yet
- Benefits of A Food Supplement Containing Boswellia Serrata and Bromelain For Improving The Quality of Life in Patients With Osteoarthritis: A Pilot Study - 2019Document7 pagesBenefits of A Food Supplement Containing Boswellia Serrata and Bromelain For Improving The Quality of Life in Patients With Osteoarthritis: A Pilot Study - 2019ranasoftNo ratings yet