You might also like
- 1malnutrition As Health ProblemDocument37 pages1malnutrition As Health ProblemIntan Sahara BachsinNo ratings yet
- Rina La Distia Nora. September 2021 JACINDocument46 pagesRina La Distia Nora. September 2021 JACINMuliaNo ratings yet
- Acute Diarrhea: Dr. Yati Soenarto, PH.D, SP - AKDocument46 pagesAcute Diarrhea: Dr. Yati Soenarto, PH.D, SP - AKadystiNo ratings yet
- What Clinicians Need To Know About Johnson & Johnson's Janssen COVID-19 VaccineDocument40 pagesWhat Clinicians Need To Know About Johnson & Johnson's Janssen COVID-19 VaccineRamahari SihalNo ratings yet
- Childbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyDocument54 pagesChildbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyVeronica MendozaNo ratings yet
- Nadeen NNNDocument46 pagesNadeen NNNHhh UuuNo ratings yet
- FrequencyDocument7 pagesFrequencysawsanNo ratings yet
- CQI HIM August 2021 PRHDocument16 pagesCQI HIM August 2021 PRHAbdur Rashid KhanNo ratings yet
- Placenta Akreta Screening and DiagnosisDocument46 pagesPlacenta Akreta Screening and DiagnosisDwiweirkepPetNo ratings yet
- Social Work Concentrating at Making Desired Improvements To A Community's Social Health, Well-Being, and Overall FunctioningDocument17 pagesSocial Work Concentrating at Making Desired Improvements To A Community's Social Health, Well-Being, and Overall FunctioningJaylord VerazonNo ratings yet
- Dr. Arto Yuwono Soeroto's Recommendations on Covid-19 VaccinationDocument35 pagesDr. Arto Yuwono Soeroto's Recommendations on Covid-19 VaccinationekaNo ratings yet
- Germany: No Data Available No Data AvailableDocument1 pageGermany: No Data Available No Data AvailableJpr Kca MjtrNo ratings yet
- Essential Newborn Care - From Evidence To PracticeDocument71 pagesEssential Newborn Care - From Evidence To PracticeReden LorenzoNo ratings yet
- TosoDocument21 pagesTosoXiomara Lizeth Intor HuaripataNo ratings yet
- Factors Predicting Relapse in Pediatric Nephrotic SyndromeDocument2 pagesFactors Predicting Relapse in Pediatric Nephrotic SyndromeVeronika runtungNo ratings yet
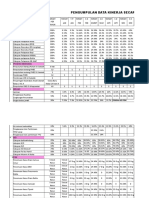
- Pengumpulan Data Kinerja Secara Periodik Tahun 2018Document6 pagesPengumpulan Data Kinerja Secara Periodik Tahun 2018rusdiyantiNo ratings yet
- Newborn CareDocument57 pagesNewborn CareDIPENDRA KUMAR KUSHAWAHANo ratings yet
- Essential Newborn CareDocument54 pagesEssential Newborn CareBrigitte CovarrubiasNo ratings yet
- TABEL RANGKUMAN FIX-dikonversi-dikonversiDocument2 pagesTABEL RANGKUMAN FIX-dikonversi-dikonversiVeronika runtungNo ratings yet
- Sri Lanka: No Data Available No Data AvailableDocument1 pageSri Lanka: No Data Available No Data AvailablePragith WijeratnamNo ratings yet
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalDocument4 pagesA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanNo ratings yet
- NAP (Harry P.) PDFDocument29 pagesNAP (Harry P.) PDFaldyNo ratings yet
- MMR Reg-Blok 2-Variasi proses-AUDocument34 pagesMMR Reg-Blok 2-Variasi proses-AUismail ajiNo ratings yet
- September Ward AuditDocument5 pagesSeptember Ward AuditJhessie ChingNo ratings yet
- Module 5&6 Statistics AnswerDocument10 pagesModule 5&6 Statistics AnswerElaine Canasta75% (4)
- School Nursing: Camarines Sur Polytechnic CollegesDocument20 pagesSchool Nursing: Camarines Sur Polytechnic CollegesMaiden MendezNo ratings yet
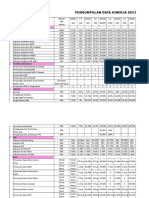
- Pengumpulan Data Kinerja Secara Periodik Tahun 2018Document6 pagesPengumpulan Data Kinerja Secara Periodik Tahun 2018rusdiyantiNo ratings yet
- Kuliah DIARE AKUT Pengantar SDocument29 pagesKuliah DIARE AKUT Pengantar SKarima Iffani UlifahNo ratings yet
- CCO 2017 NASH Quiz Anstee DownloadableDocument42 pagesCCO 2017 NASH Quiz Anstee DownloadablePD18No ratings yet
- Observations & ResultsDocument14 pagesObservations & ResultsavnishNo ratings yet
- Brief T.B. Control ProgrammeDocument3 pagesBrief T.B. Control ProgrammeAbdullah AfzalNo ratings yet
- CHN Print 1Document9 pagesCHN Print 1Fredderich LagañaNo ratings yet
- Seizures and Angelman Syndrome Thiele Study ResultsDocument11 pagesSeizures and Angelman Syndrome Thiele Study Resultsbaba ababNo ratings yet
- Medex Test Clinical Trials Results 13-05-07Document2 pagesMedex Test Clinical Trials Results 13-05-07Adir BrilNo ratings yet
- Essential Newborn Care: From Evidence To Practice: Maria Asuncion Silvestre, MD, FPSNBM, FaapDocument84 pagesEssential Newborn Care: From Evidence To Practice: Maria Asuncion Silvestre, MD, FPSNBM, FaapShane Lim GarciaNo ratings yet
- Rajendra NagarDocument20 pagesRajendra NagarBabita DhruwNo ratings yet
- HIV Prevention in Malaysia: A Brief OverviewDocument36 pagesHIV Prevention in Malaysia: A Brief OverviewyaneemayNo ratings yet
- Global Dan Nasional Problem AMR 2019Document36 pagesGlobal Dan Nasional Problem AMR 2019DewiNo ratings yet
- Abdominopelvic TB 3Document64 pagesAbdominopelvic TB 3jessaNo ratings yet
- A Practical Approach To Preventing Child Deaths: What The Pediatrician Can DoDocument44 pagesA Practical Approach To Preventing Child Deaths: What The Pediatrician Can DoSophia Loraine Dorone JesuraNo ratings yet
- EXTRACT GUAVA LEAF (Psidium Guajava) As LARVACHIDAL For Aedes AlbopictusDocument12 pagesEXTRACT GUAVA LEAF (Psidium Guajava) As LARVACHIDAL For Aedes Albopictusmitras labiroNo ratings yet
- CAstV KELong AAAP 2017 PDFDocument16 pagesCAstV KELong AAAP 2017 PDFJimeno Franscisco de los pozosNo ratings yet
- Rational Use of Medication in Constipation: Dr. Fatima Safira Alatas, PHD, Spa (K)Document32 pagesRational Use of Medication in Constipation: Dr. Fatima Safira Alatas, PHD, Spa (K)jls17dNo ratings yet
- Dma en PDFDocument1 pageDma en PDFElijah DavidNo ratings yet
- Grafik Excel 21Document13 pagesGrafik Excel 21ICUNo ratings yet
- Presentation and Analysis of DataDocument9 pagesPresentation and Analysis of DataMarge EscarchaNo ratings yet
- Tatalaksana Diare Akut Rasional Pada AnakDocument62 pagesTatalaksana Diare Akut Rasional Pada AnakMila AstariNo ratings yet
- Paper PPT Edited 20.4Document24 pagesPaper PPT Edited 20.4shruti kumarNo ratings yet
- JRPoespoprodjo - Malaria Pregnancy Infant Impact - v1Document25 pagesJRPoespoprodjo - Malaria Pregnancy Infant Impact - v1Amirullah ArsyadNo ratings yet
- Ko-Infeksi Hepatitis HIV Pencegahan Dan Penanggulangannya - UNODC Okt 2010Document85 pagesKo-Infeksi Hepatitis HIV Pencegahan Dan Penanggulangannya - UNODC Okt 2010ingridNo ratings yet
- Cardio Vascular DiseasesDocument21 pagesCardio Vascular Diseasesvoruganty_vvsNo ratings yet
- Philippines: No Data Available No Data AvailableDocument1 pagePhilippines: No Data Available No Data Availablemed wardNo ratings yet
- Hubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaDocument7 pagesHubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaNaman KhalidNo ratings yet
- Berapa Lama Follow UpDocument6 pagesBerapa Lama Follow UparifNo ratings yet
- UntitledDocument14 pagesUntitledJavier PintoNo ratings yet
- ENC Lecture2Document46 pagesENC Lecture2Fachmi Putera Susila SinuratNo ratings yet
- 2016 W. Va. Overdose Fatality AnalysisDocument26 pages2016 W. Va. Overdose Fatality AnalysisAnna MooreNo ratings yet
- 2021aug Hiv Sti 101 2018 Stats v1Document66 pages2021aug Hiv Sti 101 2018 Stats v1Narendra GowdaNo ratings yet
- Program Pengendalian Resistensi Antimikroba Di Rumah SakitDocument23 pagesProgram Pengendalian Resistensi Antimikroba Di Rumah SakitYulia Wati Safitri SanjayaNo ratings yet
- Description of The StrategyDocument6 pagesDescription of The Strategyiulia9gavrisNo ratings yet
- Food Borne DiseasesDocument29 pagesFood Borne DiseasesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines67% (6)
- Neurorehabilitation in Neuro-Oncology 2019 E-BookDocument254 pagesNeurorehabilitation in Neuro-Oncology 2019 E-BookWoffe SoloNo ratings yet
- Vit K Drug StudyDocument2 pagesVit K Drug StudyKrisha AristonNo ratings yet
- Oral and Maxillo-Facial Surgery Clinic RequirementsDocument7 pagesOral and Maxillo-Facial Surgery Clinic Requirementsal gulNo ratings yet
- Case Study TabhsoDocument7 pagesCase Study TabhsoGina Barredo Bustamante100% (1)
- Echocardiographic Anatomy in The FetusDocument14 pagesEchocardiographic Anatomy in The FetusAnonymous hOHi6TZTnNo ratings yet
- GallstonesDocument17 pagesGallstonesع ب و دNo ratings yet
- BSN 1-1 Biochem Week 6Document2 pagesBSN 1-1 Biochem Week 6PAULINE KAYE QUITANNo ratings yet
- Midwifery MGT L5Document77 pagesMidwifery MGT L5MaxNo ratings yet
- Las Ro3 Final h9q3w4 8Document17 pagesLas Ro3 Final h9q3w4 8Randolf CruzNo ratings yet
- Electro PDFDocument14 pagesElectro PDFFulg de NeaNo ratings yet
- An Occupational Health & Safety Presentation For Young Workers: Storyboard and ScriptDocument21 pagesAn Occupational Health & Safety Presentation For Young Workers: Storyboard and ScriptALEN GEONo ratings yet
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic Fevernikhil00007100% (1)
- Male Genitals and Inguinal AreaDocument8 pagesMale Genitals and Inguinal AreagayleNo ratings yet
- Diabetes Mellitus Case StudyDocument5 pagesDiabetes Mellitus Case StudyRainier Rhett Concha86% (7)
- The New York Times Magazine April 10 2016 PDFDocument62 pagesThe New York Times Magazine April 10 2016 PDFAaron ScottNo ratings yet
- 2020 Eagle Practical CardiologyDocument24 pages2020 Eagle Practical CardiologyaeliasgvNo ratings yet
- Areeb Organics Tri-Fold BrochureDocument6 pagesAreeb Organics Tri-Fold Brochurerubana reazNo ratings yet
- Metabolism of Nucleic Acids: Degradation, Absorption and RegulationDocument27 pagesMetabolism of Nucleic Acids: Degradation, Absorption and RegulationIndri YaniNo ratings yet
- DGM Sample Questions - 1Document8 pagesDGM Sample Questions - 1abdulNo ratings yet
- Expanding Designed Exercise Awareness and Produced by Gregory Petrovich GrabovoiDocument5 pagesExpanding Designed Exercise Awareness and Produced by Gregory Petrovich GrabovoiManojkumar NairNo ratings yet
- 1 Administering OxygenDocument6 pages1 Administering OxygentlokingNo ratings yet
- Colds and Their BenefitsDocument105 pagesColds and Their BenefitsAlmiranteAckbarNo ratings yet
- Oral and Maxillofacial PathologyDocument79 pagesOral and Maxillofacial PathologyMai AnhNo ratings yet
- CBG Cannabinoid Benefits and EffectsDocument10 pagesCBG Cannabinoid Benefits and EffectsjohnnemanicNo ratings yet
- Obstructive Jaundice: Causes, Symptoms and DiagnosisDocument69 pagesObstructive Jaundice: Causes, Symptoms and DiagnosisAbdirazak HassanNo ratings yet
- Cannulation Camp: Basic Needle Cannulation Training For Dialysis StaffDocument7 pagesCannulation Camp: Basic Needle Cannulation Training For Dialysis Staffcharlenetan18100% (3)
- Pamantasan NG Cabuyao: College of NursingDocument78 pagesPamantasan NG Cabuyao: College of NursingissaiahnicolleNo ratings yet
- Colic Essay OutlineDocument2 pagesColic Essay OutlineSyaie SyaiedaNo ratings yet