You might also like
- COVID 19 Vaccine Comparison ChartDocument2 pagesCOVID 19 Vaccine Comparison ChartNuklear AdiwenaNo ratings yet
- I Raise The Rates - Shingles PresentationDocument32 pagesI Raise The Rates - Shingles Presentationwind archerNo ratings yet
- Comparatie Radioterapie Adjuvantă-Radioterapie de SalvareDocument11 pagesComparatie Radioterapie Adjuvantă-Radioterapie de SalvareconionicNo ratings yet
- Patofisiologi Kanker RahimDocument98 pagesPatofisiologi Kanker RahimOjo Nesu100% (1)
- 1.3.3 Diarrhea-4 Januari-3 JanDocument56 pages1.3.3 Diarrhea-4 Januari-3 JanmaryamNo ratings yet
- Acrabstracts Org Abstract Safety of Hydroxychloroquine Withdrawal in Older Adults With Systemic Lupus Erythematosus PDFDocument3 pagesAcrabstracts Org Abstract Safety of Hydroxychloroquine Withdrawal in Older Adults With Systemic Lupus Erythematosus PDFarie ZogsNo ratings yet
- What Is Vaccine Efficacy and Why Is It Important?Document5 pagesWhat Is Vaccine Efficacy and Why Is It Important?Darshan gohilNo ratings yet
- Seizures and Angelman Syndrome Thiele Study ResultsDocument11 pagesSeizures and Angelman Syndrome Thiele Study Resultsbaba ababNo ratings yet
- Simon-Kucher - Better-Health-Report 2023-LightDocument27 pagesSimon-Kucher - Better-Health-Report 2023-LightLong Nguyễn HoàngNo ratings yet
- Psoriasis Biologics RegistryDocument6 pagesPsoriasis Biologics RegistryWei Sheng ChongNo ratings yet
- Teaching Vaccine Communication StylesDocument13 pagesTeaching Vaccine Communication StylesDakuro A EthanNo ratings yet
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalDocument4 pagesA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanNo ratings yet
- Dr. Arto Yuwono Soeroto's Recommendations on Covid-19 VaccinationDocument35 pagesDr. Arto Yuwono Soeroto's Recommendations on Covid-19 VaccinationekaNo ratings yet
- CCO Madrid 2017 Highlights SlidesetDocument52 pagesCCO Madrid 2017 Highlights SlidesetAgustin Fau MaravillaNo ratings yet
- Zika Virus Disease IshareDocument32 pagesZika Virus Disease IshareRyan Michael OducadoNo ratings yet
- Eclampsia: An Enigma: Chitra JoshiDocument4 pagesEclampsia: An Enigma: Chitra JoshiM Haris Yoga IswantoroNo ratings yet
- Gadget Addiction and The Effect of Sleep Habit, Stress, Physical Activity To ObesityDocument8 pagesGadget Addiction and The Effect of Sleep Habit, Stress, Physical Activity To ObesitySangaree ThayanithiNo ratings yet
- Effect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialDocument24 pagesEffect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialRiyan W. PratamaNo ratings yet
- Case Processing SummaryDocument4 pagesCase Processing SummaryLuthfi LazuardiNo ratings yet
- Novel Coronavirus (COVID-19) : Updates For Clinicians: September 4, 2020Document44 pagesNovel Coronavirus (COVID-19) : Updates For Clinicians: September 4, 2020Mahita SainiNo ratings yet
- Dermatologic Therapy Volume Issue 2020 (Doi 10.1111 - dth.13488) Keeling, Elizabeth Daly, Selene McKenna, Dermot B. - Dermatology Patientsâ - Knowledge and Concerns Regarding Their ImmunomodulatoryDocument8 pagesDermatologic Therapy Volume Issue 2020 (Doi 10.1111 - dth.13488) Keeling, Elizabeth Daly, Selene McKenna, Dermot B. - Dermatology Patientsâ - Knowledge and Concerns Regarding Their ImmunomodulatoryJoNo ratings yet
- Efficacy and Tolerability of Eslicarbazepine Acetate As Monotherapy in Patients of Newly Diagnosed Focal EpilepsyDocument6 pagesEfficacy and Tolerability of Eslicarbazepine Acetate As Monotherapy in Patients of Newly Diagnosed Focal EpilepsyIJAR JOURNALNo ratings yet
- Pharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeDocument3 pagesPharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeiajpsNo ratings yet
- Bacteriological Profile DR Neeharika FinalDocument15 pagesBacteriological Profile DR Neeharika FinalNiharika ShivashankarNo ratings yet
- Kepatuhan VL Anak SamarindaDocument5 pagesKepatuhan VL Anak Samarindaummi hanifNo ratings yet
- Manuscript Vulvar CancerDocument5 pagesManuscript Vulvar CancerYudha GanesaNo ratings yet
- Breast Cancer: Diagnosis and TreatmentDocument41 pagesBreast Cancer: Diagnosis and TreatmentAnggun Permata Sari SuknaNo ratings yet
- Evaluation of Postpartum Female Sterilizations: A Retrospective Study at Tertiary Care Hospital in JammuDocument6 pagesEvaluation of Postpartum Female Sterilizations: A Retrospective Study at Tertiary Care Hospital in JammuIJAR JOURNALNo ratings yet
- Indicative Target TemplateDocument11 pagesIndicative Target TemplateMulugeta DagneNo ratings yet
- Hubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaDocument7 pagesHubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaNaman KhalidNo ratings yet
- Eu 021 PDFDocument9 pagesEu 021 PDFempower93 empower93No ratings yet
- 366-Article Text-1782-1-10-20230930Document6 pages366-Article Text-1782-1-10-20230930Elang kurniati Elang kurniatiNo ratings yet
- PN PDFDocument59 pagesPN PDFAmit PatelNo ratings yet
- 2017 Vax ScaleDocument9 pages2017 Vax ScaleDragana DsNo ratings yet
- Social Work Concentrating at Making Desired Improvements To A Community's Social Health, Well-Being, and Overall FunctioningDocument17 pagesSocial Work Concentrating at Making Desired Improvements To A Community's Social Health, Well-Being, and Overall FunctioningJaylord VerazonNo ratings yet
- Data Analysis and Interpretation of HIV KnowledgeDocument23 pagesData Analysis and Interpretation of HIV KnowledgeKaryl CanaresNo ratings yet
- Egypt Steps Survey 2017 Facts and FiguresDocument2 pagesEgypt Steps Survey 2017 Facts and Figuressep 2680No ratings yet
- Egypt STEPS Survey 2017 Facts and FiguresDocument2 pagesEgypt STEPS Survey 2017 Facts and FiguresMira AhmedNo ratings yet
- Output FixDocument7 pagesOutput FixMerry NildaweniNo ratings yet
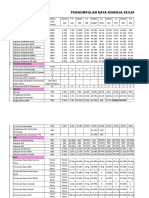
- Pengumpulan Data Kinerja Secara Periodik Tahun 2018Document6 pagesPengumpulan Data Kinerja Secara Periodik Tahun 2018rusdiyantiNo ratings yet
- Rina La Distia Nora. September 2021 JACINDocument46 pagesRina La Distia Nora. September 2021 JACINMuliaNo ratings yet
- Crosstabulation Analysis of Factors Related to Drug PreventionDocument12 pagesCrosstabulation Analysis of Factors Related to Drug PreventionMontaviana gale jamuraNo ratings yet
- Adverse Cutaneous Drug Reactions (Acdrs) in Sardjito General HospitalDocument122 pagesAdverse Cutaneous Drug Reactions (Acdrs) in Sardjito General HospitalOpung HokiNo ratings yet
- 2021aug Hiv Sti 101 2018 Stats v1Document66 pages2021aug Hiv Sti 101 2018 Stats v1Narendra GowdaNo ratings yet
- A Study On The Efficacy of Immunotherapy With Purified Protein Derivative For The Treatment of Recalcitrant WartsDocument5 pagesA Study On The Efficacy of Immunotherapy With Purified Protein Derivative For The Treatment of Recalcitrant WartsAlfian Faisal Abu JusufNo ratings yet
- The Relationship Between Sleep Quality and Students' Acne Vulgaris Severity at Medical Faculty Universitas Kristen IndonesiaDocument10 pagesThe Relationship Between Sleep Quality and Students' Acne Vulgaris Severity at Medical Faculty Universitas Kristen IndonesiaDevi MugihartiniNo ratings yet
- Effect of Papilloma Virus On Some Immunological and Molecular Traits of Infected Women in Al-Diwaniyah GovernorateDocument6 pagesEffect of Papilloma Virus On Some Immunological and Molecular Traits of Infected Women in Al-Diwaniyah GovernorateCentral Asian StudiesNo ratings yet
- Rituximab For Severe Membranous Nephropathy: A 6-Month Trial With Extended Follow-UpDocument11 pagesRituximab For Severe Membranous Nephropathy: A 6-Month Trial With Extended Follow-UpNarinder SharmaNo ratings yet
- Scenario of Retinoblastoma Among Bangladeshi Children - A Single Center Experience of 10 YearsDocument5 pagesScenario of Retinoblastoma Among Bangladeshi Children - A Single Center Experience of 10 YearsBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- Quality of Life, Respiratory Symptoms, and Health Care Utilization 1 Year Following Outpatient Management of COVID 19: A Prospective Cohort StudyDocument4 pagesQuality of Life, Respiratory Symptoms, and Health Care Utilization 1 Year Following Outpatient Management of COVID 19: A Prospective Cohort StudyFranklin GuamanNo ratings yet
- Karakteristik Faktor Siklus MenstruasiDocument7 pagesKarakteristik Faktor Siklus MenstruasiMerry NildaweniNo ratings yet
- School Nursing: Camarines Sur Polytechnic CollegesDocument20 pagesSchool Nursing: Camarines Sur Polytechnic CollegesMaiden MendezNo ratings yet
- Proportion of Specific Factors Risk of Breast Cancer On Women AGE 25-65 YEARSDocument10 pagesProportion of Specific Factors Risk of Breast Cancer On Women AGE 25-65 YEARSMichaella AlmirahNo ratings yet
- 02 Study Day 2016 - Severe Obesity Study Interim FindingsDocument26 pages02 Study Day 2016 - Severe Obesity Study Interim Findingsvrajesh pandhiNo ratings yet
- TABEL RANGKUMAN FIX-dikonversi-dikonversiDocument2 pagesTABEL RANGKUMAN FIX-dikonversi-dikonversiVeronika runtungNo ratings yet
- Laboratory Abnormalities in Patients with COVID-19Document4 pagesLaboratory Abnormalities in Patients with COVID-19Angelica Ferrer TrujequeNo ratings yet
- Dark - Field Microscopic Analysis On The Blood of 1,006 Symptomatic Persons After Anti-Covid Mrna Injections From Pfizer/Biontech or ModernaDocument60 pagesDark - Field Microscopic Analysis On The Blood of 1,006 Symptomatic Persons After Anti-Covid Mrna Injections From Pfizer/Biontech or Modernasum wunNo ratings yet
- Pain and Pain Management in ThalDocument36 pagesPain and Pain Management in ThalKavirNivNo ratings yet
- Factors Predicting Relapse in Pediatric Nephrotic SyndromeDocument2 pagesFactors Predicting Relapse in Pediatric Nephrotic SyndromeVeronika runtungNo ratings yet
- Pre-Anaesthetic Self Assessment FormDocument2 pagesPre-Anaesthetic Self Assessment FormmmmmNo ratings yet
- History of DentistryDocument24 pagesHistory of DentistryEzhilarasi INo ratings yet
- Homeopathy ProjectDocument3 pagesHomeopathy Projectapi-546805978No ratings yet
- Introduction To Hoac II, ICF-RPS & OutcomeDocument40 pagesIntroduction To Hoac II, ICF-RPS & OutcomeKC MutiaNo ratings yet
- International Observership ProgramDocument51 pagesInternational Observership ProgramSedaka DonaldsonNo ratings yet
- Clinical Study Start-Up ActivitiesDocument5 pagesClinical Study Start-Up ActivitiesMary Angelique BanogonNo ratings yet
- Astm F770-18Document4 pagesAstm F770-18Martin Tapankov100% (1)
- Nature of Fraud and Its Effects in The Medical Insurance KenyaDocument12 pagesNature of Fraud and Its Effects in The Medical Insurance KenyaSaarah ConnieNo ratings yet
- Evaluating TB Programs in Indonesian Health CentersDocument7 pagesEvaluating TB Programs in Indonesian Health CentersArnawa I PutuNo ratings yet
- Basic Surgical Techniques IllustratedDocument49 pagesBasic Surgical Techniques Illustratedromeo rivera100% (3)
- Syringe Packs BrochureDocument2 pagesSyringe Packs BrochureIrinel BuscaNo ratings yet
- 1 - A Framework For Maternal and Child Health NursingDocument3 pages1 - A Framework For Maternal and Child Health NursingShanealle Athaliah Magsalay CuaNo ratings yet
- HBS07060 Medical Interns Guide to Application and AppointmentDocument63 pagesHBS07060 Medical Interns Guide to Application and Appointmentfaraaz94No ratings yet
- PalmarDocument5 pagesPalmarshenric1667% (3)
- Hotel LeadsDocument17 pagesHotel Leadssanakausar.5089No ratings yet
- Getinge Hs33 Hospital SterilizerDocument8 pagesGetinge Hs33 Hospital SterilizerGhozy AnamNo ratings yet
- MCH ProgrammeDocument14 pagesMCH ProgrammepriyankaNo ratings yet
- Generic Drugs in The U.S.: Generic Market and Registration ChallengesDocument70 pagesGeneric Drugs in The U.S.: Generic Market and Registration ChallengesboddarambabuNo ratings yet
- Train The Trainer Manual PDFDocument146 pagesTrain The Trainer Manual PDFFootball Club AllianzNo ratings yet
- Patient Decision Aid PDF 243780159 PDFDocument23 pagesPatient Decision Aid PDF 243780159 PDFJimboNo ratings yet
- Shah 2000Document4 pagesShah 2000Ardian AshadiNo ratings yet
- Appa BrochureDocument2 pagesAppa BrochureRaghava AkshintalaNo ratings yet
- Hospitals' EmailsDocument8 pagesHospitals' EmailsAkil eswarNo ratings yet
- Philippine Airlines Flight Surgeon Not Guilty of Abandonment for Leaving Clinic to Have DinnerDocument1 pagePhilippine Airlines Flight Surgeon Not Guilty of Abandonment for Leaving Clinic to Have DinnerAlec VenturaNo ratings yet
- List of Medical Abbreviations - Latin Abbreviations - WikipediaDocument3 pagesList of Medical Abbreviations - Latin Abbreviations - WikipediaMohamed IbrahimNo ratings yet
- Health Management Information System - Tamil Nadu Case: Group 7Document17 pagesHealth Management Information System - Tamil Nadu Case: Group 7Vipul BhagatNo ratings yet
- A Review of Chronic Pain After Inguinal HerniorrhaphyDocument7 pagesA Review of Chronic Pain After Inguinal HerniorrhaphyStefano FizNo ratings yet
- Understanding Health Care Quality, Access and Policy DeterminantsDocument17 pagesUnderstanding Health Care Quality, Access and Policy DeterminantsCharley WatebaNo ratings yet
- Everything You Wanted To Know About Smart Cities - The Internet of Things Is The BackboneDocument11 pagesEverything You Wanted To Know About Smart Cities - The Internet of Things Is The BackboneGuilherme LiraNo ratings yet
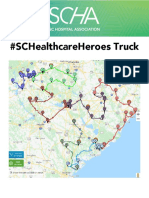
- SCHA SC Healthcare Heroes Truck Map 2020Document14 pagesSCHA SC Healthcare Heroes Truck Map 2020WIS NewsNo ratings yet