You might also like
- Pembrolizumab MonographDocument8 pagesPembrolizumab MonographpmuftiaNo ratings yet
- What Clinicians Need To Know About Johnson & Johnson's Janssen COVID-19 VaccineDocument40 pagesWhat Clinicians Need To Know About Johnson & Johnson's Janssen COVID-19 VaccineRamahari SihalNo ratings yet
- 2028-Article Text-9832-3-10-20131105Document3 pages2028-Article Text-9832-3-10-20131105HMC ProcurementNo ratings yet
- Full TextDocument4 pagesFull TextAlfa FebriandaNo ratings yet
- A Case Series of Metastatic Lateral Cervical LymphadenopathyDocument5 pagesA Case Series of Metastatic Lateral Cervical LymphadenopathyKriti KumariNo ratings yet
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalDocument4 pagesA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanNo ratings yet
- Wikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)Document4 pagesWikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)jcasanovas1995No ratings yet
- Kohan 2011Document10 pagesKohan 2011David DwiputeraNo ratings yet
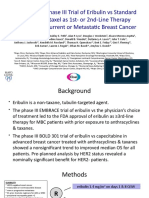
- Randomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast CancerDocument14 pagesRandomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast Canceralberto cabelloNo ratings yet
- School Nursing: Camarines Sur Polytechnic CollegesDocument20 pagesSchool Nursing: Camarines Sur Polytechnic CollegesMaiden MendezNo ratings yet
- Trastuzumab MonographDocument11 pagesTrastuzumab MonographAmeliaNo ratings yet
- 1.3.3 Diarrhea-4 Januari-3 JanDocument56 pages1.3.3 Diarrhea-4 Januari-3 JanmaryamNo ratings yet
- Presentation 1 FinalDocument13 pagesPresentation 1 FinalJeetendra SahNo ratings yet
- j.1528-1167.2006.00715 30.xDocument272 pagesj.1528-1167.2006.00715 30.xJeremy PorteousNo ratings yet
- 2020 Epilepsy With Myoclonic-Atonic Seizures (Doose Syndrome)Document8 pages2020 Epilepsy With Myoclonic-Atonic Seizures (Doose Syndrome)Florian LamblinNo ratings yet
- 1 s2.0 S1059131198900103 MainDocument4 pages1 s2.0 S1059131198900103 MainPutu Filla JfNo ratings yet
- Boehringer Ingelheim Page 11 of 14 Trajenta Linagliptin, 5 MG Film Coated Tablet Response DocumentDocument1 pageBoehringer Ingelheim Page 11 of 14 Trajenta Linagliptin, 5 MG Film Coated Tablet Response DocumentHendra Wana Nur'aminNo ratings yet
- Sjs Ten KuchingDocument54 pagesSjs Ten KuchingChuaMinHuangNo ratings yet
- Diabetic Neuropathy RCT (Diacon 2017)Document17 pagesDiabetic Neuropathy RCT (Diacon 2017)Prof. Dr. Manishkumar PatelNo ratings yet
- Chiron Et Al 2011 EpilepsiaDocument4 pagesChiron Et Al 2011 EpilepsiaAlexandra PrikopNo ratings yet
- Clinioepidemiological Features of Epilepsy in The Aral RegionDocument6 pagesClinioepidemiological Features of Epilepsy in The Aral RegionCentral Asian StudiesNo ratings yet
- Analgesic Use by Leprosy Patients': Volume 54, Number 3Document4 pagesAnalgesic Use by Leprosy Patients': Volume 54, Number 3imeNo ratings yet
- Refractory EpilepsyDocument17 pagesRefractory EpilepsyAngga M RahmanNo ratings yet
- Main 71Document6 pagesMain 71pokharelriwaj82No ratings yet
- Epilepsy in ChildrenDocument34 pagesEpilepsy in ChildrenAdam MochtarNo ratings yet
- 008Document3 pages008indriNo ratings yet
- 2023 Evaluating The Relationship of Skin InvolvementDocument1 page2023 Evaluating The Relationship of Skin InvolvementDiego melo limaNo ratings yet
- Seizures and Epilepsy:: ClassificationDocument26 pagesSeizures and Epilepsy:: ClassificationNollanoleNo ratings yet
- Community Acquired Pneumonia, Lancet, 12-03Document11 pagesCommunity Acquired Pneumonia, Lancet, 12-03Maya ramadaniNo ratings yet
- A Comparative Study of Complications of Vivax and Falciparum Malaria in Dehradun, IndiaDocument5 pagesA Comparative Study of Complications of Vivax and Falciparum Malaria in Dehradun, IndiaUDNo ratings yet
- Scientific Letter: Archivos de Bronconeumología 58 (2022) T457-T460Document4 pagesScientific Letter: Archivos de Bronconeumología 58 (2022) T457-T460johannaNo ratings yet
- Pharmacovigilance Q1 Summary 20232024Document19 pagesPharmacovigilance Q1 Summary 20232024Dharmendra KumarNo ratings yet
- Artigo Envelhecimento PolifarmáciaDocument5 pagesArtigo Envelhecimento Polifarmáciadjonatan zuffoNo ratings yet
- Use of Aeds in 2011 and Beyond: Optimizing Clinical ManagementDocument32 pagesUse of Aeds in 2011 and Beyond: Optimizing Clinical ManagementchandanNo ratings yet
- Myelopathy Due To Cervical Spondylosis in Yaoundé: Clinical Features and TreatmentDocument4 pagesMyelopathy Due To Cervical Spondylosis in Yaoundé: Clinical Features and TreatmentNasrullah nsrNo ratings yet
- Macroprolactinomas in Children and Adolescents - Factors Associated With The Response To Treatment in 77 PatientsDocument10 pagesMacroprolactinomas in Children and Adolescents - Factors Associated With The Response To Treatment in 77 Patientsmelany.sanchezNo ratings yet
- 427 EndoDocument9 pages427 EndoBioq. GallegosNo ratings yet
- Oligomenoragia PDFDocument8 pagesOligomenoragia PDFsjhfksglakdjalfsfNo ratings yet
- GRINDEM Epidemiologic Survey of Thrombocytopenia in DogsDocument6 pagesGRINDEM Epidemiologic Survey of Thrombocytopenia in DogsElle Burton-BradleyNo ratings yet
- The Impact of Genetic Variations in ADORA2A in The Association Between Caffeine Consumption and SleepDocument17 pagesThe Impact of Genetic Variations in ADORA2A in The Association Between Caffeine Consumption and SleepnutrinathyalvesNo ratings yet
- Sekeres MDS ASH TraineeDocument63 pagesSekeres MDS ASH TraineeИван НегарэNo ratings yet
- 60d587530e3c120210625article - PDF - FileStudy of Maternal and Perinatal OutcomDocument4 pages60d587530e3c120210625article - PDF - FileStudy of Maternal and Perinatal Outcommade dharmaNo ratings yet
- Long-Term Effectiveness and Tolerability of Topiramate in Children With Epilepsy Under The Age of 2 Years: 4-Year Follow-UpDocument7 pagesLong-Term Effectiveness and Tolerability of Topiramate in Children With Epilepsy Under The Age of 2 Years: 4-Year Follow-Uppkarina_3No ratings yet
- Epilepsy & Behavior: Betul Baykan, Iris E. Martínez-Juárez, Ebru A. Altindag, Carol S. Cam Field, Peter R. Cam FieldDocument7 pagesEpilepsy & Behavior: Betul Baykan, Iris E. Martínez-Juárez, Ebru A. Altindag, Carol S. Cam Field, Peter R. Cam Fieldnyrypk8wpqNo ratings yet
- Professional Information BrochureDocument16 pagesProfessional Information BrochureKane SmithNo ratings yet
- Pharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeDocument3 pagesPharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeiajpsNo ratings yet
- Chromosome 1p36 DeletionsDocument4 pagesChromosome 1p36 Deletionsericwang12No ratings yet
- Diagnostic and Prognostic Value of Anamnesis in Adolescent Girls With Disordered Menstrual ActivityDocument8 pagesDiagnostic and Prognostic Value of Anamnesis in Adolescent Girls With Disordered Menstrual ActivityCentral Asian StudiesNo ratings yet
- Thrombolytics: Interventional FellowDocument51 pagesThrombolytics: Interventional Fellowusfcards100% (1)
- Gaptg 6Document3 pagesGaptg 6DIKE NOVELLA -No ratings yet
- LockdownDocument5 pagesLockdownArpana HazarikaNo ratings yet
- 10.1016@S0140 67360560746 5Document2 pages10.1016@S0140 67360560746 5SakinaNo ratings yet
- Remarkably High Efficacy of Cenobamate in Adults With Focal-Onset Seizures: A Double-Blind, Randomized, Placebo-Controlled TrialDocument3 pagesRemarkably High Efficacy of Cenobamate in Adults With Focal-Onset Seizures: A Double-Blind, Randomized, Placebo-Controlled TrialDiana LeonNo ratings yet
- Efficacy and Tolerability of Eslicarbazepine Acetate As Monotherapy in Patients of Newly Diagnosed Focal EpilepsyDocument6 pagesEfficacy and Tolerability of Eslicarbazepine Acetate As Monotherapy in Patients of Newly Diagnosed Focal EpilepsyIJAR JOURNALNo ratings yet
- The Landscape of Epilepsy-Related GATOR1 Variants Baldassari 2019Document11 pagesThe Landscape of Epilepsy-Related GATOR1 Variants Baldassari 2019cicasmileNo ratings yet
- Evaluation of The Clinical Efficacy of Phenytoin in The Treatment of Epileptic Seizures in ChildrenDocument4 pagesEvaluation of The Clinical Efficacy of Phenytoin in The Treatment of Epileptic Seizures in ChildrenAcademic JournalNo ratings yet
- SCN1A Seizure Disorders Encompass A Spectrum That Ranges FromDocument27 pagesSCN1A Seizure Disorders Encompass A Spectrum That Ranges FromDavidTiagoMukaseyNo ratings yet
- Papier EpilepsieDocument5 pagesPapier EpilepsieCelebre MualabaNo ratings yet
- Angiogenic Profile Identifies Pulmonary Hypertension in Children With Down SyndromeDocument8 pagesAngiogenic Profile Identifies Pulmonary Hypertension in Children With Down Syndromebaba ababNo ratings yet
- HHS Public Access: Endocrine Manifestations of Down SyndromeDocument11 pagesHHS Public Access: Endocrine Manifestations of Down Syndromebaba ababNo ratings yet
- Role of Executive Function in Developmental Stuttering Nihms-1062016Document19 pagesRole of Executive Function in Developmental Stuttering Nihms-1062016baba ababNo ratings yet
- Epilepsy in Angelman Syndrome: A Scoping Review: Debopam SamantaDocument13 pagesEpilepsy in Angelman Syndrome: A Scoping Review: Debopam Samantababa ababNo ratings yet
- COVID 19 Associated Vasculitis and Vasculopathy: Richard C. BeckerDocument13 pagesCOVID 19 Associated Vasculitis and Vasculopathy: Richard C. Beckerbaba ababNo ratings yet
- Epilepsy in Angelman Syndrome: Karine Pelc, Stewart G. Boyd, Guy Cheron, Bernard DanDocument7 pagesEpilepsy in Angelman Syndrome: Karine Pelc, Stewart G. Boyd, Guy Cheron, Bernard Danbaba ababNo ratings yet
- Stuttering Treatment and Its PharmacologyDocument8 pagesStuttering Treatment and Its Pharmacologybaba ababNo ratings yet
- Neurocognition of Developmental Disorders of Language Ullman2017Document29 pagesNeurocognition of Developmental Disorders of Language Ullman2017baba ababNo ratings yet
- Neuromagnetic Oscillations in Sensory Systems Stuttering Epilepsy STB 2019Document13 pagesNeuromagnetic Oscillations in Sensory Systems Stuttering Epilepsy STB 2019baba ababNo ratings yet
- Cortico-Basal GGL Thalamcort Loop Development StutteringDocument15 pagesCortico-Basal GGL Thalamcort Loop Development Stutteringbaba ababNo ratings yet
- The Abnormal EEG: Background AbnormalitiesDocument33 pagesThe Abnormal EEG: Background Abnormalitiesbaba ababNo ratings yet
- Epilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-AnalysisDocument9 pagesEpilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-Analysisbaba ababNo ratings yet
- Origin and Technical Aspects of The EEGDocument37 pagesOrigin and Technical Aspects of The EEGbaba ababNo ratings yet
- February Outpatient Clinics - AmbrusDocument1 pageFebruary Outpatient Clinics - Ambrusbaba ababNo ratings yet
- Pedstroke2017ajnr A5376 FullDocument8 pagesPedstroke2017ajnr A5376 Fullbaba ababNo ratings yet
- Banking Financial InstitutionsDocument252 pagesBanking Financial Institutionspraise ferrerNo ratings yet
- Modes of Flexible LearningDocument4 pagesModes of Flexible LearningJesseilou GullebanNo ratings yet
- Proposal 4psDocument6 pagesProposal 4psCaridad Avila67% (3)
- ReportDocument10 pagesReportNeeraj KishoreNo ratings yet
- 11th Bio Botany Important Questions For Volume 1 PDFDocument6 pages11th Bio Botany Important Questions For Volume 1 PDFNaren44% (9)
- I - Infowatch 16-30 Jun 2023Document141 pagesI - Infowatch 16-30 Jun 2023Suman MondalNo ratings yet
- Tomato BankDocument67 pagesTomato Bankkmusatheek musatheekNo ratings yet
- Capital Budgeting Practices by Corporates in India PPTDocument13 pagesCapital Budgeting Practices by Corporates in India PPTRVijaySai0% (1)
- Veolia Case StudyDocument15 pagesVeolia Case StudyKanakarao MalappareddyNo ratings yet
- A&D MGMU End Sem Exam Paper (2022-23) Part-IDocument5 pagesA&D MGMU End Sem Exam Paper (2022-23) Part-IAzar BargirNo ratings yet
- Wind Seismic CalculationsDocument4 pagesWind Seismic Calculationsumesh0% (1)
- NEB Syllabus For Class 12 Science PhysicsDocument4 pagesNEB Syllabus For Class 12 Science Physicskumar HarshNo ratings yet
- ConclusionDocument1 pageConclusionArun GuptaNo ratings yet
- India: "Truth Alone Triumphs"Document103 pagesIndia: "Truth Alone Triumphs"Rajesh NaiduNo ratings yet
- Hybrid Solar Chimney With Salt Water Desalination and Power GenerationDocument4 pagesHybrid Solar Chimney With Salt Water Desalination and Power GenerationAishwaryaNo ratings yet
- Hadoop Course Content PDFDocument9 pagesHadoop Course Content PDFNaveen ElancersoftNo ratings yet
- CSN-261: Data Structures Laboratory: Lab Assignment 5 (L5)Document3 pagesCSN-261: Data Structures Laboratory: Lab Assignment 5 (L5)GajananNo ratings yet
- Aubrey Jaffer: Scheme Implementation Version 5f1Document149 pagesAubrey Jaffer: Scheme Implementation Version 5f1kevinmcguireNo ratings yet
- Dzone Refcard 292 Advanced Kubernetes 2020 PDFDocument9 pagesDzone Refcard 292 Advanced Kubernetes 2020 PDFLeonardo Moreno ForeroNo ratings yet
- The Sniper - Storey PDFDocument177 pagesThe Sniper - Storey PDFJose Luis95% (19)
- Alxion: For Direct DriveDocument56 pagesAlxion: For Direct DriveAnselmo Aguado cortesNo ratings yet
- How To Product ManualDocument250 pagesHow To Product ManualAmith M DNo ratings yet
- Islamic Private Debt Securities (Ipds)Document37 pagesIslamic Private Debt Securities (Ipds)Sara IbrahimNo ratings yet
- Induction Motor NotesDocument20 pagesInduction Motor NotesMani SaiNo ratings yet
- Drawing List: Infrastructure / 7100 - MV Power Duct Network Rev. NoDocument2 pagesDrawing List: Infrastructure / 7100 - MV Power Duct Network Rev. NosayedNo ratings yet
- LTE Throughput Troubleshooting GuidlelineDocument15 pagesLTE Throughput Troubleshooting GuidlelineTourchianNo ratings yet
- DEH-1250MPG DEH-1250MP: Owner's Manual Manual de Instrucciones Manual Do ProprietárioDocument80 pagesDEH-1250MPG DEH-1250MP: Owner's Manual Manual de Instrucciones Manual Do ProprietárioMoezz Asif Research Associate-Faculty of Avionics EngineeringNo ratings yet
- Sheet #6 Ensemble + Neural Nets + Linear Regression + Backpropagation + CNNDocument4 pagesSheet #6 Ensemble + Neural Nets + Linear Regression + Backpropagation + CNNrowaida elsayedNo ratings yet
- Full Report XeriaDocument11 pagesFull Report XeriaHamierul MohamadNo ratings yet
- Sachet MarketingDocument7 pagesSachet MarketingTom JohnNo ratings yet