You might also like
- Easy Guide To MiasmaticsDocument12 pagesEasy Guide To Miasmaticsdbsmanian100% (1)
- Identifying VariablesDocument4 pagesIdentifying VariablesAllan CastroNo ratings yet
- Original PDF Medical Terminology Complete 4th Edition PDFDocument41 pagesOriginal PDF Medical Terminology Complete 4th Edition PDFmegan.soffel782100% (35)
- MPN GenomicsDocument1 pageMPN GenomicsTejus BehlNo ratings yet
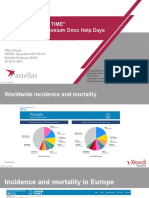
- Onco Help Days 26-28.11.2021 Dr. MurgDocument37 pagesOnco Help Days 26-28.11.2021 Dr. MurgCorina-Maria BoticiNo ratings yet
- Molecular Minimal Residual Disease Detection in Acute Myeloid LeukemiaDocument42 pagesMolecular Minimal Residual Disease Detection in Acute Myeloid LeukemiaANo ratings yet
- aCML Where Are We NowDocument17 pagesaCML Where Are We NowShayne Tee-MelegritoNo ratings yet
- 09 - Chapter 3Document18 pages09 - Chapter 3The FrequencyNo ratings yet
- Lo Coco FrancescoDocument61 pagesLo Coco FrancescoJess silvaNo ratings yet
- Excli 17 159 PDFDocument10 pagesExcli 17 159 PDFEko RistiyantoNo ratings yet
- VIP Cives Oncotarget 2016Document16 pagesVIP Cives Oncotarget 2016Jemma ArakelyanNo ratings yet
- Seizures and Angelman Syndrome Thiele Study ResultsDocument11 pagesSeizures and Angelman Syndrome Thiele Study Resultsbaba ababNo ratings yet
- 2016 NGS Predictive of FIBROSISDocument12 pages2016 NGS Predictive of FIBROSISmaomaochongNo ratings yet
- Adpkd CursDocument56 pagesAdpkd Cursplaiul mioriticNo ratings yet
- Afib For JCU 2Document33 pagesAfib For JCU 2Sofia KusumadewiNo ratings yet
- Sjs Ten KuchingDocument54 pagesSjs Ten KuchingChuaMinHuangNo ratings yet
- MDS MPN2019 DR Rachel SalitDocument39 pagesMDS MPN2019 DR Rachel Salitluca.win92No ratings yet
- AsundexianDocument25 pagesAsundexianshahane musayelyanNo ratings yet
- Cerebrovscular DiseasesDocument28 pagesCerebrovscular DiseasesbagussofianNo ratings yet
- Arrythmia Management in Primary CareDocument51 pagesArrythmia Management in Primary CarecelinamannaNo ratings yet
- 10 1016@j Ajhg 2019 04 014Document8 pages10 1016@j Ajhg 2019 04 014Ifany oschaliaNo ratings yet
- Early Detection of Chronic Kidney Disease in Primary Healthcare - Dr. ChandraDocument27 pagesEarly Detection of Chronic Kidney Disease in Primary Healthcare - Dr. Chandrabellaayunda putriNo ratings yet
- Anticoagulation in Atrial FibrillationDocument22 pagesAnticoagulation in Atrial FibrillationprobowurNo ratings yet
- AfibDocument91 pagesAfibreyNo ratings yet
- Paediatric AML Guidance Dec 2015Document33 pagesPaediatric AML Guidance Dec 2015Genetic Clinic UKMNo ratings yet
- Myelodysplastic SyndromeDocument27 pagesMyelodysplastic SyndromeWesley MugambiNo ratings yet
- Myelodysplastic Syndrome: DR Mika Lumbantobing, Sppd-KhomDocument20 pagesMyelodysplastic Syndrome: DR Mika Lumbantobing, Sppd-KhomsehatkabauNo ratings yet
- Myelodysplastic Syndromes: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDocument15 pagesMyelodysplastic Syndromes: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpUmmul HayatiNo ratings yet
- Rimmer SPEP Multiple MyelomaDocument35 pagesRimmer SPEP Multiple MyelomaAaron AntonioNo ratings yet
- Prostrate CancerDocument63 pagesProstrate CancereviltohuntNo ratings yet
- Trastuzumab MonographDocument11 pagesTrastuzumab MonographAmeliaNo ratings yet
- LSD Shed Light On Lysosomal Dysfunction in Parkinsons Disease (12p)Document12 pagesLSD Shed Light On Lysosomal Dysfunction in Parkinsons Disease (12p)noam aradNo ratings yet
- Dapa Brief Data (14271)Document24 pagesDapa Brief Data (14271)Adel SALLAM100% (1)
- Thrombolytics: Interventional FellowDocument51 pagesThrombolytics: Interventional Fellowusfcards100% (1)
- CML PresentationDocument55 pagesCML PresentationИван НегарэNo ratings yet
- Multiple Myeloma A New Treatment ApproachDocument27 pagesMultiple Myeloma A New Treatment ApproachIndonesian Journal of Cancer100% (1)
- Pharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeDocument3 pagesPharmaceutical Sciences: Recent Advances and Treatments of Childhood Nephrotic SyndromeiajpsNo ratings yet
- 12 ON 2020 Lung WBDocument96 pages12 ON 2020 Lung WBabdullahNo ratings yet
- When To Obtain Genomic Data in Acute Myeloid Leukemia (AML) and Which Mutations MatterDocument11 pagesWhen To Obtain Genomic Data in Acute Myeloid Leukemia (AML) and Which Mutations MatterEnrique GuerreroNo ratings yet
- CvotDocument29 pagesCvotakash kondapalliNo ratings yet
- Expression Profiling of Metastatic Renal Cell Carcinoma Using Gene Set Enrichment AnalysisDocument6 pagesExpression Profiling of Metastatic Renal Cell Carcinoma Using Gene Set Enrichment AnalysisPradnya GNo ratings yet
- YA CCO - IO - in - Urothelial - Cancer - Downloadable - 1Document27 pagesYA CCO - IO - in - Urothelial - Cancer - Downloadable - 1Yasar HammorNo ratings yet
- BRACAADocument16 pagesBRACAAotmane.elbriniNo ratings yet
- CCO 2020 WCLC Downloadable 1Document106 pagesCCO 2020 WCLC Downloadable 1Florencia GuerraNo ratings yet
- P ' R O R N 2008: Epidemiology/EtiologyDocument17 pagesP ' R O R N 2008: Epidemiology/EtiologyDiana MitreaNo ratings yet
- Understanding Multiple Myeloma and Laboratory ValuesDocument25 pagesUnderstanding Multiple Myeloma and Laboratory ValuesMeena Tiwari100% (1)
- Multiple MyelomaDocument40 pagesMultiple MyelomaJayelle2100% (1)
- Atorvastatin Statin in CVD ManagementDocument37 pagesAtorvastatin Statin in CVD ManagementSriNo ratings yet
- Statins in CVD Management: Is Just Lipid Lowering Enough?Document37 pagesStatins in CVD Management: Is Just Lipid Lowering Enough?SriNo ratings yet
- Who 2016Document35 pagesWho 2016Herlina InaNo ratings yet
- TWILIGHT DM AjitDocument21 pagesTWILIGHT DM Ajitajit jadhavNo ratings yet
- Aml Patho Physiology & Classification - V RocchaDocument61 pagesAml Patho Physiology & Classification - V RocchaThuy NguyenNo ratings yet
- The Management of Metastatic GIST: Current Standard and Investigational TherapeuticsDocument12 pagesThe Management of Metastatic GIST: Current Standard and Investigational Therapeuticsbawoji1763No ratings yet
- Mds Case Study: 80-Year-Old Female With Macrocytic AnemiaDocument24 pagesMds Case Study: 80-Year-Old Female With Macrocytic AnemiaNor Lainie MonawaraNo ratings yet
- Leukemia Panel Sample ReportDocument2 pagesLeukemia Panel Sample ReportAnmol DubeyNo ratings yet
- Leukemia Panel Sample ReportDocument2 pagesLeukemia Panel Sample ReportAnmol DubeyNo ratings yet
- Leukemia Panel Sample Report 2Document2 pagesLeukemia Panel Sample Report 2kurd kar2No ratings yet
- Myelodysplastic Syndromes1Document26 pagesMyelodysplastic Syndromes1api-205355237No ratings yet
- Revised International Prognostic Scoring System (IPSS-R) : Developed by The International Working Group For Prognosis in MDS (IWG-PM)Document23 pagesRevised International Prognostic Scoring System (IPSS-R) : Developed by The International Working Group For Prognosis in MDS (IWG-PM)Sri IriantiNo ratings yet
- Association of Soluble Suppression of Tumorigenesis-2 (ST2) With Endothelial Function in Patients With Ischemic Heart FailureDocument11 pagesAssociation of Soluble Suppression of Tumorigenesis-2 (ST2) With Endothelial Function in Patients With Ischemic Heart Failurere septian IlhamsyahNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Fast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondFrom EverandFast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondNo ratings yet
- HLH-2020-ASH TalkDocument43 pagesHLH-2020-ASH TalkИван НегарэNo ratings yet
- ASH Hematology Review Series - Hodgkin Lymphoma - HerreraDocument69 pagesASH Hematology Review Series - Hodgkin Lymphoma - HerreraИван НегарэNo ratings yet
- ASH Hematology Review Series - Indolent LymphomasDocument77 pagesASH Hematology Review Series - Indolent LymphomasИван НегарэNo ratings yet
- T Cell Lymphomas 2022 SlidesDocument62 pagesT Cell Lymphomas 2022 SlidesИван НегарэNo ratings yet
- Mullally - ASH Hematology Review Series - MPN - CombinedDocument40 pagesMullally - ASH Hematology Review Series - MPN - CombinedИван НегарэNo ratings yet
- WM ASH Hematology Review Series 6-2022Document64 pagesWM ASH Hematology Review Series 6-2022Иван НегарэNo ratings yet
- ASH Hematology Review Series - AML - Sallman D - 6-2022Document60 pagesASH Hematology Review Series - AML - Sallman D - 6-2022Иван НегарэNo ratings yet
- Hepatic InvolvementDocument8 pagesHepatic InvolvementИван НегарэNo ratings yet
- Angels in America Audience GuideDocument30 pagesAngels in America Audience Guidedurkin44100% (2)
- Trends in Molecular Medicine - December 2013Document51 pagesTrends in Molecular Medicine - December 2013Kevin SavouryNo ratings yet
- Clinicopathological Study of Hashimoto Thyroiditis: Pooja Jain, Geetha Vasudevan, Kanthilata PaiDocument5 pagesClinicopathological Study of Hashimoto Thyroiditis: Pooja Jain, Geetha Vasudevan, Kanthilata PaiRifqi Fathul ArroisiNo ratings yet
- Paces Notes SC 2017Document38 pagesPaces Notes SC 2017subhankar100% (3)
- Star Super Surplus Floater BrochureDocument5 pagesStar Super Surplus Floater BrochurepunNo ratings yet
- 1.D/D of Intraconal Mass 2.D/D of Leucocoria 3.U/S & CT Findings of RB 4.how Will You Manage That CaseDocument15 pages1.D/D of Intraconal Mass 2.D/D of Leucocoria 3.U/S & CT Findings of RB 4.how Will You Manage That CaseMuhammad SharjeelNo ratings yet
- Gadtc PHCDocument246 pagesGadtc PHCshawnNo ratings yet
- Ulcerative Colitis in ChildrenDocument5 pagesUlcerative Colitis in ChildrentheservantNo ratings yet
- Thoracos PDFDocument40 pagesThoracos PDFmanjunath kalal100% (1)
- Neuroblastoma PDFDocument5 pagesNeuroblastoma PDFHanna G. FauziaNo ratings yet
- Leukocoria 2016Document35 pagesLeukocoria 2016DiskaAstarini100% (1)
- Conective Issue Massage PDFDocument3 pagesConective Issue Massage PDFSergio Andres ZeitgeistNo ratings yet
- TRM05.03 Blunt Abdominal Trauma Guideline V2 - 08.17Document7 pagesTRM05.03 Blunt Abdominal Trauma Guideline V2 - 08.17Erwin WibowoNo ratings yet
- Medical Terminology For Medical Transcription TraineesDocument74 pagesMedical Terminology For Medical Transcription TraineesRangothri Sreenivasa SubramanyamNo ratings yet
- Same Sex Adoption EvDocument5 pagesSame Sex Adoption Evapi-292471795No ratings yet
- Ignatavicius TOCDocument9 pagesIgnatavicius TOCjennaaahhhNo ratings yet
- Care of The Clients With Eye and Ear DisorderDocument35 pagesCare of The Clients With Eye and Ear DisorderKristine Joy RevañoNo ratings yet
- Advanced Special Subject 9.2Document22 pagesAdvanced Special Subject 9.2Nguyen Ngoc Khoi NguyenNo ratings yet
- Liver Abscesses and CystsDocument6 pagesLiver Abscesses and CystsbintangsebayangNo ratings yet
- Damage Control Management y Polytrauma PatientDocument324 pagesDamage Control Management y Polytrauma PatientMauri ParadedaNo ratings yet
- Blood Donation: SMJK Kwang Hua, Klang Project Base Learning 2Document8 pagesBlood Donation: SMJK Kwang Hua, Klang Project Base Learning 2LOOK YU QI MoeNo ratings yet
- CCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormDocument1 pageCCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormMigori ArtNo ratings yet
- Thyroglossal Duct Cyst in The Suprasternal RegionDocument3 pagesThyroglossal Duct Cyst in The Suprasternal RegionKhairuman anandaNo ratings yet
- Ratio - Assessment Exam Np1Document29 pagesRatio - Assessment Exam Np1Ian Mizzel A. DulfinaNo ratings yet
- Interna Prof. Djanggan - Kapita SelektaDocument53 pagesInterna Prof. Djanggan - Kapita SelektaNur Laily MardianaNo ratings yet
- Psoriasis & Mgt.Document70 pagesPsoriasis & Mgt.kurutalaNo ratings yet
- General Pathology 4.03 Endocrine System Super SummaryDocument15 pagesGeneral Pathology 4.03 Endocrine System Super SummaryJade MonrealNo ratings yet