You might also like
- UntitledDocument306 pagesUntitledmonica100% (5)
- Question Tag SlideDocument33 pagesQuestion Tag SlidekwanphylNo ratings yet
- 27 - CC SAN ANTONIO - Hypothyroidism, Hyper, Thyroid Nodular Disease and CancerDocument77 pages27 - CC SAN ANTONIO - Hypothyroidism, Hyper, Thyroid Nodular Disease and CancerDann San AntonioNo ratings yet
- Hyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeDocument54 pagesHyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeMegan MendozaNo ratings yet
- Pathophysiology of Endocrine SystemDocument64 pagesPathophysiology of Endocrine SystemTess MohamedNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkkyNo ratings yet
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- 4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFDocument89 pages4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFjackie funtanilla100% (1)
- Hormon GDSDocument23 pagesHormon GDSBRI KUNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Thyroid PathophysiologyDocument7 pagesThyroid PathophysiologyS RiarNo ratings yet
- Thyroid GlandDocument30 pagesThyroid GlandahmedkomranNo ratings yet
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- Pharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsDocument48 pagesPharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsAmanuel MaruNo ratings yet
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocument38 pagesSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Hypothyroidism in PregnancyDocument29 pagesHypothyroidism in PregnancyhanaddulNo ratings yet
- Thyroid DisordersDocument21 pagesThyroid DisordersSuliman GarallehNo ratings yet
- Thyroid DX PXLDocument62 pagesThyroid DX PXLabduljebarNo ratings yet
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocument36 pagesThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNo ratings yet
- Thyroid and InfertilityDocument36 pagesThyroid and InfertilitySairindri SahooNo ratings yet
- Thyroid GlandDocument127 pagesThyroid GlandCarla Mae MoraNo ratings yet
- Hyperprolactinem IaDocument63 pagesHyperprolactinem Iakhadzx100% (2)
- Powerpoint: Disorders of The Thyroid GlandDocument67 pagesPowerpoint: Disorders of The Thyroid Glandj.doe.hex_87100% (1)
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- TPO in PregnancyDocument18 pagesTPO in PregnancyRoxana TudorNo ratings yet
- Pemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKDocument12 pagesPemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKBonitavanyNo ratings yet
- Drug Management of Thyroid DiseaseDocument22 pagesDrug Management of Thyroid DiseaseHassan.shehri100% (6)
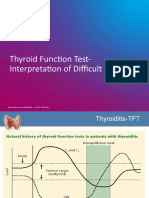
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- HyperthyroidismDocument40 pagesHyperthyroidismmypublicidNo ratings yet
- Endocrine Disorders 1234399857677955 1Document130 pagesEndocrine Disorders 1234399857677955 1api-19824701No ratings yet
- Hyperthyroidism: A Practical Approach To Diagnosis and ManagementDocument70 pagesHyperthyroidism: A Practical Approach To Diagnosis and ManagementMutiara Manuella TambaNo ratings yet
- Thyroid Emergencies: Abrar AlharbiDocument35 pagesThyroid Emergencies: Abrar AlharbiabrarNo ratings yet
- Thyroid Disorders During PregnancyDocument25 pagesThyroid Disorders During PregnancyA.H.ANo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Pathology of Thyroid GlandDocument138 pagesPathology of Thyroid GlandAhsan KazmiNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Thyroid HormonesDocument7 pagesThyroid HormonesAbdullah EssaNo ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Pathophysiology of Endocrine SystemDocument37 pagesPathophysiology of Endocrine SystemRodriguez Vivanco Kevin DanielNo ratings yet
- Physiology of The Thyroid GlandDocument28 pagesPhysiology of The Thyroid GlandSecret AgentNo ratings yet
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- Grave'S Disease: Farida Ulfa 1510211057Document11 pagesGrave'S Disease: Farida Ulfa 1510211057farida ulfaNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- Conference Brochure With Link7Document16 pagesConference Brochure With Link7Shrutik AshiyaniNo ratings yet
- Im Testing For Endocrine DisordersDocument7 pagesIm Testing For Endocrine DisordersChristine MendozaNo ratings yet
- Hyperthyroidism History TakingDocument11 pagesHyperthyroidism History TakingmokkailinNo ratings yet
- Thyroid DisordersDocument34 pagesThyroid DisordersAbdulhameed Mohamed100% (1)
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- Parathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Document28 pagesParathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Omar Alruwaili100% (1)
- Hyperthyroidsm: EpidemiologyDocument6 pagesHyperthyroidsm: EpidemiologyEllieNo ratings yet
- Week 3 Pharmaco Part 2Document34 pagesWeek 3 Pharmaco Part 2Tiko JomidavaNo ratings yet
- Adrenal and Pitutary Disoreders Adigrat LecDocument144 pagesAdrenal and Pitutary Disoreders Adigrat Lecbereket gashuNo ratings yet
- Disorders of The Thyroid and Parathyroid Glands: Ms TeamDocument36 pagesDisorders of The Thyroid and Parathyroid Glands: Ms TeamShy Dela PuertaNo ratings yet
- How To Interpret Thyroid Function TestsDocument5 pagesHow To Interpret Thyroid Function TestsnonieshzNo ratings yet
- MKSAP13-Hematology and OncologyDocument261 pagesMKSAP13-Hematology and OncologyimanNo ratings yet
- Drug Toxicity and PoisoningDocument12 pagesDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDONo ratings yet
- Thyroid Disease in PregnancyDocument53 pagesThyroid Disease in PregnancyTee Wei SianNo ratings yet
- Pathology of ThyroidDocument59 pagesPathology of ThyroidDavid Curtis Mintah100% (1)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- OSCE ReviewDocument45 pagesOSCE ReviewKay BristolNo ratings yet
- Bipolar Disorder: Best Practices in Screening, Diagnosis and TreatmentDocument51 pagesBipolar Disorder: Best Practices in Screening, Diagnosis and TreatmentKay BristolNo ratings yet
- Nephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassDocument143 pagesNephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassKay BristolNo ratings yet
- Management of Type 2 Diabetes and Its ChallengesDocument81 pagesManagement of Type 2 Diabetes and Its ChallengesKay BristolNo ratings yet
- 2007 Nov 07 CompleteDocument62 pages2007 Nov 07 CompleteKay BristolNo ratings yet
- 2007 MAY JUNE 2007 CompleteDocument68 pages2007 MAY JUNE 2007 CompleteKay BristolNo ratings yet
- Anaemia in PregnancyDocument5 pagesAnaemia in PregnancyKay BristolNo ratings yet
- Pub HLT Ckik VDocument8 pagesPub HLT Ckik VKay BristolNo ratings yet
- Anaesthesia Clerkship HandbookDocument12 pagesAnaesthesia Clerkship HandbookKay BristolNo ratings yet
- AIRWAY MANAGEMENT (Clinical Anaesthesiology 5 Ed. by M & M)Document30 pagesAIRWAY MANAGEMENT (Clinical Anaesthesiology 5 Ed. by M & M)Kay BristolNo ratings yet
- Definition:: IschemicDocument4 pagesDefinition:: IschemicKay BristolNo ratings yet
- Laryngoscope: 1. Handle and BladeDocument8 pagesLaryngoscope: 1. Handle and BladeKay BristolNo ratings yet
- Paymanager Process: To Mapping of PostsDocument6 pagesPaymanager Process: To Mapping of PostspksolNo ratings yet
- Shane P. Prejean, MD, Munaib Din, BSC, Eliana Reyes, MD, PHD, and Fadi G. Hage, MD, FasncDocument8 pagesShane P. Prejean, MD, Munaib Din, BSC, Eliana Reyes, MD, PHD, and Fadi G. Hage, MD, FasncwidyadariNo ratings yet
- The Quick Stacking Word Game: For To PlayersDocument12 pagesThe Quick Stacking Word Game: For To PlayersMark BallingerNo ratings yet
- The Four Confidences EbookDocument38 pagesThe Four Confidences EbookIgor PopadicNo ratings yet
- CGI Programming in CDocument27 pagesCGI Programming in CPiya BaradNo ratings yet
- Bài tập 1: Chọn đúng thì của các câu sau (quá khứ đơn và quá khứ tiếp diễn)Document24 pagesBài tập 1: Chọn đúng thì của các câu sau (quá khứ đơn và quá khứ tiếp diễn)Thị Thu Hà BùiNo ratings yet
- NavrasDocument2 pagesNavrasAayushi PandeyNo ratings yet
- A Historical Examination of Concrete PDFDocument324 pagesA Historical Examination of Concrete PDFMa Ria Fe100% (1)
- Ansys 18.2: Transient Analysis On The BridgeDocument7 pagesAnsys 18.2: Transient Analysis On The BridgeUsman Khalil50% (2)
- PostgreSQL Functions by ExampleDocument41 pagesPostgreSQL Functions by ExampleNguyễn Đăng HưngNo ratings yet
- Additional Science / Biology: Bl2Hp Mark SchemeDocument13 pagesAdditional Science / Biology: Bl2Hp Mark SchemeMrs S BakerNo ratings yet
- D.C Circuits Class TestDocument1 pageD.C Circuits Class TestShinde JayakrishnaNo ratings yet
- Paper Neupogen PDFDocument13 pagesPaper Neupogen PDFFranNo ratings yet
- The Filipino WayDocument21 pagesThe Filipino WayMel Belisario TubeoNo ratings yet
- LearnEnglish Reading C1 Four Book SummariesDocument5 pagesLearnEnglish Reading C1 Four Book SummariesGeorge YounesNo ratings yet
- Essential Formulas For Algebra 2 Final Exam PDFDocument10 pagesEssential Formulas For Algebra 2 Final Exam PDFJustin JeudyNo ratings yet
- Englishs Journal Ahmad MukhlasDocument5 pagesEnglishs Journal Ahmad MukhlasAdelia PuspaNo ratings yet
- Dire Dawa Institute of Technology Department of Construction Technology and Management COTM6041-Construction Law and ContractDocument147 pagesDire Dawa Institute of Technology Department of Construction Technology and Management COTM6041-Construction Law and ContractAshenafi shamenaNo ratings yet
- 8th Grades-Unit 8 Worksheet - by Mete - EltDocument2 pages8th Grades-Unit 8 Worksheet - by Mete - EltEce GunesNo ratings yet
- Wordlist Unit 5Document3 pagesWordlist Unit 5Anastasiia SokolovaNo ratings yet
- CTAP For NGFW - Data Privacy NoticeDocument3 pagesCTAP For NGFW - Data Privacy NoticeGiovanni -No ratings yet
- The Poetic Process and The Poetic GeniusDocument6 pagesThe Poetic Process and The Poetic Geniusadeloptera100% (2)
- The Second or St. Thomas's Gospel of The Infancy of Jesus ChristDocument3 pagesThe Second or St. Thomas's Gospel of The Infancy of Jesus ChristHat RedNo ratings yet
- Sauvage - Essays On Anglophone Poetry by Richard Owens Book PreviewDocument36 pagesSauvage - Essays On Anglophone Poetry by Richard Owens Book PreviewBlazeVOX [books]No ratings yet
- 577-Article Text-847-1-10-20220207Document10 pages577-Article Text-847-1-10-20220207Ikhwanul AnsarNo ratings yet
- Micro, Small and Medium Enterprises Survey in Nigeria by SmedanDocument182 pagesMicro, Small and Medium Enterprises Survey in Nigeria by Smedanleye02100% (2)
- Group 10 Battle of SiffinDocument2 pagesGroup 10 Battle of SiffinMuhammad IbrahimNo ratings yet
- 6-Month Probationary Employee Performance EvaluationDocument2 pages6-Month Probationary Employee Performance EvaluationmbabluNo ratings yet