You might also like
- Meridians Organs SymptomsDocument23 pagesMeridians Organs SymptomsFlorina Stefan100% (2)
- Pediatric Critical Care, 3rd Edition 2009 DR - NaggarDocument389 pagesPediatric Critical Care, 3rd Edition 2009 DR - NaggarmariamNo ratings yet
- Castro CellSaltsHandoutsDocument19 pagesCastro CellSaltsHandoutsShubhankar Bhowmick100% (4)
- Psychotropic Drugs & ChildrenDocument6 pagesPsychotropic Drugs & ChildrenART.ASNNo ratings yet
- Hemoflagellates PDFDocument69 pagesHemoflagellates PDFIzzah AtqaNo ratings yet
- Lone Gammeltoft, Marianne Sollok Nordenhof - Autism, Play and Social Interaction-Jessica Kingsley Pub (2008) PDFDocument212 pagesLone Gammeltoft, Marianne Sollok Nordenhof - Autism, Play and Social Interaction-Jessica Kingsley Pub (2008) PDFLudmilaCândidoNo ratings yet
- Olanzapine Vs AripiprazoleDocument8 pagesOlanzapine Vs AripiprazoleDivaviyaNo ratings yet
- HAHNEMANN S., Materia Medica PuraDocument1,145 pagesHAHNEMANN S., Materia Medica PuraJayesh TalekarNo ratings yet
- 1949 Bonaparte Life and Works of Edgar Allen PoeDocument773 pages1949 Bonaparte Life and Works of Edgar Allen PoeTsniaga Seman100% (15)
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
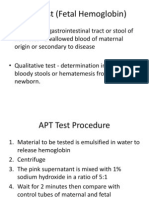
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- Case Report MTH HydroceleDocument9 pagesCase Report MTH Hydrocelesamuel_hildaNo ratings yet
- Cancer Case StudyDocument23 pagesCancer Case StudyMeynard AndresNo ratings yet
- Buku AJar Infeksi Dan Pediatrik Tropis IDAIDocument31 pagesBuku AJar Infeksi Dan Pediatrik Tropis IDAIAndika SiswantaNo ratings yet
- Tabel Konversi FiO2Document2 pagesTabel Konversi FiO2arie_yuliantoNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- Hipertiroid HarrisonDocument8 pagesHipertiroid HarrisonravenskaNo ratings yet
- HDDocument23 pagesHDSardjitoNo ratings yet
- Ca GasterDocument27 pagesCa GastermerryNo ratings yet
- Mallory Weiss TearDocument12 pagesMallory Weiss TeararshadmunNo ratings yet
- Osteonecrosis Caput FemurDocument23 pagesOsteonecrosis Caput FemurdrhendyjuniorNo ratings yet
- Children With Henoch Schonlein Purpura 2.0Document13 pagesChildren With Henoch Schonlein Purpura 2.0soniaNo ratings yet
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilNo ratings yet
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaNo ratings yet
- Help CfponsetiDocument32 pagesHelp CfponsetiShAi_MyStERiOuSNo ratings yet
- Nervus Laryngeus RecurrensDocument5 pagesNervus Laryngeus RecurrensAri Julian SaputraNo ratings yet
- Cerebral Malaria Diagnosis & TreatmentDocument42 pagesCerebral Malaria Diagnosis & TreatmentLivia HanisamurtiNo ratings yet
- Retinopati DiabetikDocument5 pagesRetinopati DiabetikMuhammad Afriadi HamdanNo ratings yet
- Lapsus Susp - Ca EndometriumDocument22 pagesLapsus Susp - Ca Endometriumjeams manuNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- Malignant Soft Tissue TumorsDocument21 pagesMalignant Soft Tissue TumorsEva GustianiNo ratings yet
- Hubungan Beberapa Indikator Obesitas Dengan Kadar Asam UratDocument17 pagesHubungan Beberapa Indikator Obesitas Dengan Kadar Asam UratarbiantoniNo ratings yet
- Non Traditional Family Life CycleDocument2 pagesNon Traditional Family Life CycleIshan Dutta100% (1)
- Systemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesDocument30 pagesSystemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesOrion JohnNo ratings yet
- Boys Chart Arm Circumference For Age3 Months To 5 Years (Percentiles)Document1 pageBoys Chart Arm Circumference For Age3 Months To 5 Years (Percentiles)Rahmawati Nur AzizahNo ratings yet
- Deskripsi MurmurDocument3 pagesDeskripsi MurmurLevina Tri RatanaNo ratings yet
- Congenital Adrenal HyperplasiaDocument2 pagesCongenital Adrenal HyperplasiaesyNo ratings yet
- Perdarahan Varises GasterDocument8 pagesPerdarahan Varises Gastermandala22No ratings yet
- Jurnal Forensik Trauma KimiaDocument5 pagesJurnal Forensik Trauma Kimiaikram hanafiNo ratings yet
- Open Fracture Phalanx Distal Digiti IV Manus Dextra With Open Fracture Phalanx Medial Digiti II Hearts SynthesisDocument6 pagesOpen Fracture Phalanx Distal Digiti IV Manus Dextra With Open Fracture Phalanx Medial Digiti II Hearts SynthesisYusri YudhaNo ratings yet
- Trantornos Anorrectales Adquiridos PDFDocument7 pagesTrantornos Anorrectales Adquiridos PDFIván Castellares RojasNo ratings yet
- LAPKAS PLASENTA AKRETA FINAL EDIT PageDocument84 pagesLAPKAS PLASENTA AKRETA FINAL EDIT Pagemuttaqin95No ratings yet
- Tanda dan Komplikasi Perforasi Usus pada Demam TifoidDocument5 pagesTanda dan Komplikasi Perforasi Usus pada Demam TifoidSisca Dwi Agustina0% (1)
- Hydranencephaly: A Rare Cause of An Enlarging Head Size in An InfantDocument3 pagesHydranencephaly: A Rare Cause of An Enlarging Head Size in An InfantdyahNo ratings yet
- Oeis SyndromeDocument9 pagesOeis SyndromeADEENo ratings yet
- Disentri Et Causa Bacteria: Jl. Kutai Raya, Perumnas-3, Tangerang Kecamatan Curug, Kab. Tangerang, Provinsi Banten)Document14 pagesDisentri Et Causa Bacteria: Jl. Kutai Raya, Perumnas-3, Tangerang Kecamatan Curug, Kab. Tangerang, Provinsi Banten)Denny LeeNo ratings yet
- tuGAS KILOTHORAXDocument25 pagestuGAS KILOTHORAXAlma WijayaNo ratings yet
- Struma Nodusa: Pembimbing: Dr. Rizapahlevi., M.Si., SP.BDocument45 pagesStruma Nodusa: Pembimbing: Dr. Rizapahlevi., M.Si., SP.BAndre Pradnyana100% (1)
- Juvenile Idiopathic Arthritis: An Update On PharmacotherapyDocument13 pagesJuvenile Idiopathic Arthritis: An Update On PharmacotherapyRahmi SilviyaniNo ratings yet
- Cholangiocarcinoma Differential DiagnosisDocument2 pagesCholangiocarcinoma Differential DiagnosisPremaKurniaNo ratings yet
- Tokyo Guidelines 2018 Diagnostic Criteria and Seve6706321783624012310Document15 pagesTokyo Guidelines 2018 Diagnostic Criteria and Seve6706321783624012310Katrina bangaoetNo ratings yet
- Respiratory Diseases Commonly FoundDocument29 pagesRespiratory Diseases Commonly FoundyudhaNo ratings yet
- DRUG ERUPTION GUIDEDocument46 pagesDRUG ERUPTION GUIDESyahDikaNo ratings yet
- Bunga Rampai Infeksi Dengue AnakDocument67 pagesBunga Rampai Infeksi Dengue AnakSatrio PrimaesoNo ratings yet
- Current Diagnosis and Management of Hirschsprung's DiseaseDocument20 pagesCurrent Diagnosis and Management of Hirschsprung's DiseaseIyan AsianaNo ratings yet
- Medulla Compression AcuteDocument46 pagesMedulla Compression AcuteamiraNo ratings yet
- Overview of The Mucopolysaccharidoses: RheumatologyDocument9 pagesOverview of The Mucopolysaccharidoses: RheumatologyLaura Orjuela MateusNo ratings yet
- Laporan Kasus Preeklampsia: Disusun Oleh: Dr. Muhammad Fadlan PulunganDocument1 pageLaporan Kasus Preeklampsia: Disusun Oleh: Dr. Muhammad Fadlan PulunganDebora Angelina TobingNo ratings yet
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsNo ratings yet
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- 2012RossClassificationarticleinPedCardiology PDFDocument7 pages2012RossClassificationarticleinPedCardiology PDFKumiko MichishigeNo ratings yet
- Ross 2012Document6 pagesRoss 2012Ivan VeriswanNo ratings yet
- Age-Stratified Revision of Ross Classification for Pediatric Heart FailureDocument6 pagesAge-Stratified Revision of Ross Classification for Pediatric Heart FailureCitra Eva MeilyndhaNo ratings yet
- Heart FailureDocument6 pagesHeart FailureMita RahNo ratings yet
- Barst RJ 2011 Pulmonary Arterial Hypertension A Comparison Between Children and AdultsDocument13 pagesBarst RJ 2011 Pulmonary Arterial Hypertension A Comparison Between Children and Adultsdr.herusetiawanNo ratings yet
- Angiogenic profile identifies pulmonary hypertension in children with Down syndromeDocument8 pagesAngiogenic profile identifies pulmonary hypertension in children with Down syndromebaba ababNo ratings yet
- Sleep Disordered Breathing in Bronchopulmonary DysplasiaDocument9 pagesSleep Disordered Breathing in Bronchopulmonary DysplasiaJHONATAN MATA ARANDANo ratings yet
- Strength & Difficulties Questionnaire (SDQ) - Usia 6-10 TH (Tanggapan)Document677 pagesStrength & Difficulties Questionnaire (SDQ) - Usia 6-10 TH (Tanggapan)radwika antyNo ratings yet
- Davanzo KMCProtocol JHL2013Document8 pagesDavanzo KMCProtocol JHL2013radwika antyNo ratings yet
- Bagan AnalisaDocument1 pageBagan Analisaradwika antyNo ratings yet
- Strength & Difficulties Questionnaire (SDQ) - Usia 6-10 TH (Tanggapan)Document677 pagesStrength & Difficulties Questionnaire (SDQ) - Usia 6-10 TH (Tanggapan)radwika antyNo ratings yet
- PDFDocument2 pagesPDFradwika antyNo ratings yet
- Intensive Care Nursery House Staff ManualDocument3 pagesIntensive Care Nursery House Staff ManualgalaxytwyNo ratings yet
- Pathophysio Bact MeningitisDocument19 pagesPathophysio Bact Meningitisibn_saed100% (1)
- Cellulitis Definition, Etiology, and Clinical FeaturesDocument10 pagesCellulitis Definition, Etiology, and Clinical Featuresrosscharles1006869No ratings yet
- Levels of EvidenceDocument35 pagesLevels of Evidenceradwika antyNo ratings yet
- Febrile Neutropenia: Multinational Association For Supportive Care in Cancer (MASCC)Document4 pagesFebrile Neutropenia: Multinational Association For Supportive Care in Cancer (MASCC)radwika anty100% (1)
- Levels of Evidence PDFDocument1 pageLevels of Evidence PDFRahmat AlfiansyahNo ratings yet
- Urinary Markers in The Early Stage of Nephropathy in Patients With Childhood-Onset Type 1 DiabetesDocument9 pagesUrinary Markers in The Early Stage of Nephropathy in Patients With Childhood-Onset Type 1 Diabetesradwika antyNo ratings yet
- Catherine F. HughesDocument14 pagesCatherine F. Hughesradwika antyNo ratings yet
- Promethazine Hydrochloride Tablets 25mg Usp - Taj Pharma, Leaflet Patient Medication InformationDocument3 pagesPromethazine Hydrochloride Tablets 25mg Usp - Taj Pharma, Leaflet Patient Medication InformationTAJ PHARMA — A Health Care ProviderNo ratings yet
- Wheel Chairs in India - 'Abling' The Disabled!Document60 pagesWheel Chairs in India - 'Abling' The Disabled!ssj9No ratings yet
- Hints For Remembering Medication ClassificationsDocument2 pagesHints For Remembering Medication ClassificationsSarah SNo ratings yet
- KEMH Guidelines On Cardiac Disease in PregnancyDocument7 pagesKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaNo ratings yet
- Written Report - PhilHealthDocument5 pagesWritten Report - PhilHealthSophia VeralloNo ratings yet
- Phase 1/2/3 COVID-19 Vaccine Candidate StudyDocument28 pagesPhase 1/2/3 COVID-19 Vaccine Candidate StudychamniezbuntowanyNo ratings yet
- Press Release FS Announced FINALDocument4 pagesPress Release FS Announced FINALDrDylanMNo ratings yet
- ATORVASTATINDocument1 pageATORVASTATINSHEILA MAE SACLOTNo ratings yet
- Drug Study MedicationsDocument10 pagesDrug Study Medicationsamal abdulrahmanNo ratings yet
- Per Bech: The Bech, Hamilton and Zung Scales For Mood DisordersDocument85 pagesPer Bech: The Bech, Hamilton and Zung Scales For Mood DisordersKmoespinoNo ratings yet
- Boenninghausen's Lesser Writings on HomoeopathyDocument244 pagesBoenninghausen's Lesser Writings on HomoeopathySony JohnyNo ratings yet
- Gout in CKDDocument6 pagesGout in CKDNatasya Ryani PurbaNo ratings yet
- Community Medicine Solved BCQs 8th Semester MBBS LUMHS-1Document27 pagesCommunity Medicine Solved BCQs 8th Semester MBBS LUMHS-1rameez ahmedNo ratings yet
- Aminomutase Which Converts B-Leucine Into L-Leucine and Vice-VersaDocument4 pagesAminomutase Which Converts B-Leucine Into L-Leucine and Vice-VersaYohana MariaNo ratings yet
- Sibayan, Quenna - Im AdconDocument25 pagesSibayan, Quenna - Im AdconQuenna Liza SibayanNo ratings yet
- Childhood Obesity NewsletterDocument2 pagesChildhood Obesity Newsletterapi-253381005No ratings yet
- Penicillin Drug StudyDocument2 pagesPenicillin Drug StudyEmagra AzilNo ratings yet
- Gcu Nur643e Full Course Latest 2019 September No Week 1 ReflectionDocument16 pagesGcu Nur643e Full Course Latest 2019 September No Week 1 ReflectionDoreenNo ratings yet
- Inflammatory Bowel DiseaseDocument412 pagesInflammatory Bowel DiseaseSabbra CadabraNo ratings yet
- Myocardial Infarction: Myocardial Infarction (MI) or Acute Myocardial Infarction (AMI), Commonly KnownDocument6 pagesMyocardial Infarction: Myocardial Infarction (MI) or Acute Myocardial Infarction (AMI), Commonly KnownLyka Cuanan CorcueraNo ratings yet
- Presented by DR - Asha V Sasi 2 MD CR DeptDocument32 pagesPresented by DR - Asha V Sasi 2 MD CR DeptSariIdaMihartiNo ratings yet