You might also like
- Meningitis - 2018Document55 pagesMeningitis - 2018Abraham Anaely100% (1)
- Paediatrics Notes CreatedDocument28 pagesPaediatrics Notes CreatedAbraham AnaelyNo ratings yet
- Meningitis in ChildrenDocument30 pagesMeningitis in ChildrenPNVRSNo ratings yet
- CNS InfectionDocument18 pagesCNS InfectionJason LinNo ratings yet
- Pedia MeningitisDocument1 pagePedia MeningitisiSmayli (smyle-smayl)No ratings yet
- Diplopia (Double Vision) : BackgroundDocument4 pagesDiplopia (Double Vision) : BackgroundJessica AdhykaNo ratings yet
- CSF Findings in MeningitisDocument11 pagesCSF Findings in MeningitisLioraNo ratings yet
- Outpatient Pneumonia Management Cheat SheetDocument18 pagesOutpatient Pneumonia Management Cheat SheetElaine IllescasNo ratings yet
- EBV Virus Causing Infectious MononucleosisDocument21 pagesEBV Virus Causing Infectious MononucleosiskamalNo ratings yet
- Neonatal SepsisDocument38 pagesNeonatal SepsisJavier Saad100% (1)
- Brucellosis: ClassificationDocument3 pagesBrucellosis: ClassificationAbdul-rhman AlmarshoodNo ratings yet
- Meningitis PDFDocument10 pagesMeningitis PDFAlfatahadi SNo ratings yet
- Whit Blood Cells and Benign DisordersDocument81 pagesWhit Blood Cells and Benign Disordersmichael firmanNo ratings yet
- PEDIA aPSGNDocument2 pagesPEDIA aPSGNiSmayli (smyle-smayl)No ratings yet
- Calculator Sepsis - Adhi TeguhDocument46 pagesCalculator Sepsis - Adhi TeguhBayu KurniawanNo ratings yet
- Neisse RiaDocument49 pagesNeisse RiaSubhada GosaviNo ratings yet
- Laboratory Diagnosis of MeningitisDocument28 pagesLaboratory Diagnosis of Meningitissangeetha_v100No ratings yet
- Neonatal Sepsis: Learning ObjectivesDocument10 pagesNeonatal Sepsis: Learning ObjectivesSatya Prakash TiwariNo ratings yet
- The Role of Vaccination in Salmonella ControlDocument51 pagesThe Role of Vaccination in Salmonella ControlDr. Aja Ogboo Chikere100% (1)
- Pass Ascp 2020 LatestDocument6 pagesPass Ascp 2020 LatestLorelie ChenNo ratings yet
- (K8) Sepsis Kuliah 2016Document37 pages(K8) Sepsis Kuliah 2016mayastplNo ratings yet
- LO Week 4Document6 pagesLO Week 4Jessica AdhykaNo ratings yet
- Neonatal Crohns Disease Caused by Compound Homozygous Mutation in IL 10RA A Case ReportDocument6 pagesNeonatal Crohns Disease Caused by Compound Homozygous Mutation in IL 10RA A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Acquired Heart DiseaseDocument44 pagesAcquired Heart DiseaseMedisina101No ratings yet
- Fulminant Hepatic FailureDocument53 pagesFulminant Hepatic FailureAR KarthickNo ratings yet
- clinical pathology ( body fluids) 4 semesterDocument12 pagesclinical pathology ( body fluids) 4 semesterSiddhi KaulNo ratings yet
- Beta ThalassemiaDocument36 pagesBeta ThalassemiaJyothsna JoyNo ratings yet
- Case Study Nephrotic SyndromeDocument15 pagesCase Study Nephrotic SyndromePaola Camain93% (15)
- Urinary Tract Infection: Case ReportDocument16 pagesUrinary Tract Infection: Case ReportAulia RahmanNo ratings yet
- Strepto Cocci PDFDocument34 pagesStrepto Cocci PDFMustafa SaßerNo ratings yet
- Pulmonary Infection TreatmentDocument32 pagesPulmonary Infection TreatmentKarin G. LoveraNo ratings yet
- Sepsis Recognition and TreatmentDocument33 pagesSepsis Recognition and TreatmentNhat NguyenNo ratings yet
- AntibioticsDocument13 pagesAntibioticsJOrgeNo ratings yet
- Bakteri SSPDocument69 pagesBakteri SSPCiendy ShintyaNo ratings yet
- Reoviruses, Rotaviruses, & CalcivirusesDocument3 pagesReoviruses, Rotaviruses, & CalcivirusesJoherNo ratings yet
- Difficult or Tricky Antibiotic Resistance Phenotypes To RecognizeDocument66 pagesDifficult or Tricky Antibiotic Resistance Phenotypes To Recognizetanty_ukNo ratings yet
- Iv Fluid Rate Computations: 1. DROPS PER MINUTE (Gtt/min)Document9 pagesIv Fluid Rate Computations: 1. DROPS PER MINUTE (Gtt/min)Luriel BancasoNo ratings yet
- Clinical Chemistry Tumor MarkersDocument6 pagesClinical Chemistry Tumor Markerskatherineanne.diamanteNo ratings yet
- Cep Halo Sporin SDocument9 pagesCep Halo Sporin SJasper VictoriaNo ratings yet
- MeningitisDocument44 pagesMeningitisMega Cahya VidyaningrumNo ratings yet
- Clinical Pharmacology - Rationale Behind Antibiotics PrescriptionDocument12 pagesClinical Pharmacology - Rationale Behind Antibiotics PrescriptionhalesNo ratings yet
- CSF Abnormalities in Bacterial MeningitisDocument82 pagesCSF Abnormalities in Bacterial MeningitisIulia TemuscoNo ratings yet
- Meningitis (Completed)Document26 pagesMeningitis (Completed)seema83% (6)
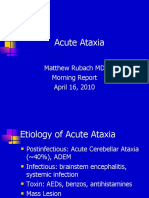
- Acute Cerebellar AtaxiaDocument8 pagesAcute Cerebellar AtaxiaEmily EresumaNo ratings yet
- ESBLDocument32 pagesESBLVenny PatriciaNo ratings yet
- Pediatric Neurologic Disorders: Syarif DarwinDocument26 pagesPediatric Neurologic Disorders: Syarif DarwinronalisaanrizNo ratings yet
- Micro CDBDocument9 pagesMicro CDBLicensed to HealNo ratings yet
- Bacterial Meningitis in NeonatesDocument3 pagesBacterial Meningitis in Neonatesyoke limuriaNo ratings yet
- Clinical Chemistry2 (Lec) Finals (TumorMarkers)Document7 pagesClinical Chemistry2 (Lec) Finals (TumorMarkers)katherineanne.diamanteNo ratings yet
- Urinary Tract Infection: Case ReportDocument17 pagesUrinary Tract Infection: Case ReportjoyNo ratings yet
- Non Malignant WBCDocument12 pagesNon Malignant WBCPALATTAO, AUBRIE L. BSMT2-8No ratings yet
- PSGNDocument23 pagesPSGNalpha mae beltranNo ratings yet
- Anti-Microbial USMLE Review: Active RecallDocument32 pagesAnti-Microbial USMLE Review: Active Recallmehrzi kamelNo ratings yet
- Hypomagnesemic Tetany in Calve1Document1 pageHypomagnesemic Tetany in Calve1Morad ImadNo ratings yet
- Emergecies in Farm AnimalsDocument31 pagesEmergecies in Farm Animalsprenume numeNo ratings yet
- Clinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Document3 pagesClinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Joey CuayoNo ratings yet
- Parasitic DiseasesDocument28 pagesParasitic DiseasesWz bel DfNo ratings yet
- Drug Study Patient SheetDocument12 pagesDrug Study Patient SheetDeborah Mae MondoyNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- InflammationDocument2 pagesInflammationBea ConstantinoNo ratings yet
- QuiapoDocument1 pageQuiapoBea ConstantinoNo ratings yet
- First Lab Exam ReviewerDocument13 pagesFirst Lab Exam ReviewerBea Constantino100% (1)
- Kas1 FinalPaperDocument8 pagesKas1 FinalPaperBea ConstantinoNo ratings yet
- Sponsors ListDocument4 pagesSponsors ListBea Constantino85% (61)
- Simulia Abaqus Standard DatasheetDocument3 pagesSimulia Abaqus Standard Datasheetuser923019231831No ratings yet
- An Introduction To Liturgy of The Catholic ChurchDocument27 pagesAn Introduction To Liturgy of The Catholic ChurchElsha DamoloNo ratings yet
- Business EnvironmentDocument12 pagesBusiness EnvironmentAbhinav GuptaNo ratings yet
- Software Client Linux 21 01Document81 pagesSoftware Client Linux 21 01BronskyNo ratings yet
- Business Analysis FoundationsDocument39 pagesBusiness Analysis FoundationsPriyankaNo ratings yet
- City MSJDocument50 pagesCity MSJHilary LedwellNo ratings yet
- 19 Unpriced BOM, Project & Manpower Plan, CompliancesDocument324 pages19 Unpriced BOM, Project & Manpower Plan, CompliancesAbhay MishraNo ratings yet
- Service Positioning and DesignDocument3 pagesService Positioning and DesignSaurabh SinhaNo ratings yet
- The Unbounded MindDocument190 pagesThe Unbounded MindXtof ErNo ratings yet
- Organic Facial Remedies Versus Inorganic Facial RemediesDocument13 pagesOrganic Facial Remedies Versus Inorganic Facial Remediesapi-271179911No ratings yet
- Admisibility To Object EvidenceDocument168 pagesAdmisibility To Object EvidenceAnonymous 4WA9UcnU2XNo ratings yet
- S06 - 1 THC560 DD311Document128 pagesS06 - 1 THC560 DD311Canchari Pariona Jhon AngelNo ratings yet
- PAPERBOARD QUALITYDocument8 pagesPAPERBOARD QUALITYaurelia carinaNo ratings yet
- Grace Lipsini1 2 3Document4 pagesGrace Lipsini1 2 3api-548923370No ratings yet
- Final - WPS PQR 86Document4 pagesFinal - WPS PQR 86Parag WadekarNo ratings yet
- Copy Resit APLC MiniAssignmentDocument5 pagesCopy Resit APLC MiniAssignmentChong yaoNo ratings yet
- European Business in China Position Paper 2017 2018 (English Version)Document408 pagesEuropean Business in China Position Paper 2017 2018 (English Version)Prasanth RajuNo ratings yet
- L Williams ResumeDocument2 pagesL Williams Resumeapi-555629186No ratings yet
- Common Pesticides in AgricultureDocument6 pagesCommon Pesticides in AgricultureBMohdIshaqNo ratings yet
- 5.a Personal Diet Consultant For Healthy MealDocument5 pages5.a Personal Diet Consultant For Healthy MealKishore SahaNo ratings yet
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- InteliLite AMF20-25Document2 pagesInteliLite AMF20-25albertooliveira100% (2)
- K230F Equipment ManualsDocument166 pagesK230F Equipment ManualsHui ChenNo ratings yet
- An Overview of The FUPLA 2 Tools: Project DatabaseDocument2 pagesAn Overview of The FUPLA 2 Tools: Project DatabaseJulio Cesar Rojas SaavedraNo ratings yet
- Cell Selection ReselectionDocument35 pagesCell Selection ReselectionThiaguNo ratings yet
- Load Frequency Control of Hydro and Nuclear Power System by PI & GA ControllerDocument6 pagesLoad Frequency Control of Hydro and Nuclear Power System by PI & GA Controllerijsret100% (1)
- BarclaysDocument5 pagesBarclaysMehul KelkarNo ratings yet
- General Biology 2-Week 2-Module 4-Evidence of EvolutionDocument16 pagesGeneral Biology 2-Week 2-Module 4-Evidence of EvolutionFEMALE Dawal LaizaNo ratings yet
- Fermat points and the Euler circleDocument2 pagesFermat points and the Euler circleKen GamingNo ratings yet