You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Test Bank For Module 6 MCQsDocument12 pagesTest Bank For Module 6 MCQsbcristoforiNo ratings yet
- Lecture-28 Placenta PreviaDocument43 pagesLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- Kartik Rangaraj. - Pathology, USMLE STEP 1, Volume 1 - Basic Pathology PDFDocument206 pagesKartik Rangaraj. - Pathology, USMLE STEP 1, Volume 1 - Basic Pathology PDFEzhil joeNo ratings yet
- Lecture-35 Eectronic Fetal MonitoringDocument45 pagesLecture-35 Eectronic Fetal MonitoringMadhu Sudhan PandeyaNo ratings yet
- Dr. Yoshimizu's Infrared Therapy Research With The Amethyst BiomatDocument2 pagesDr. Yoshimizu's Infrared Therapy Research With The Amethyst BiomatKusk29KuskNo ratings yet
- Lecture-10 EpisiotomyDocument11 pagesLecture-10 EpisiotomyMadhu Sudhan Pandeya67% (3)
- Seminar On Optic AtrophyDocument50 pagesSeminar On Optic Atrophygmc,bhopal100% (1)
- Case Analysis Group 1Document12 pagesCase Analysis Group 1mark_partolanNo ratings yet
- Lecture-33 Postpartum HemorrhageDocument50 pagesLecture-33 Postpartum HemorrhageMadhu Sudhan Pandeya100% (2)
- US NAVY Aeromedical Reference and Waiver Guide-2014Document317 pagesUS NAVY Aeromedical Reference and Waiver Guide-2014Guillermo Andres Cedron VeraNo ratings yet
- Rheumatoid ArthritisDocument44 pagesRheumatoid ArthritisBulborea Mihaela100% (1)
- Baneji PDFDocument6 pagesBaneji PDFSuraj YadavNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Boik Natural Compounds in Cancer Therapy Promising Nontoxic Antitumor Agents From Plants & Other Natural Sources (2001) PDFDocument541 pagesBoik Natural Compounds in Cancer Therapy Promising Nontoxic Antitumor Agents From Plants & Other Natural Sources (2001) PDFIoana Antonesi100% (1)
- Qi Gong - Qi Gong Therapeutic ExerciseDocument7 pagesQi Gong - Qi Gong Therapeutic Exerciseapi-3821211100% (1)
- Benign Leucocytes DisordersDocument30 pagesBenign Leucocytes DisordersNINSIIMA GERALD100% (1)
- Lecture-4 Diagnosis of PregnancyDocument31 pagesLecture-4 Diagnosis of PregnancyMadhu Sudhan Pandeya100% (1)
- Quick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountDocument2 pagesQuick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountMadhu Sudhan Pandeya100% (1)
- Voter ListDocument214 pagesVoter ListMadhu Sudhan PandeyaNo ratings yet
- Screening - Part 1Document4 pagesScreening - Part 1Madhu Sudhan PandeyaNo ratings yet
- Nepal Medical Council Act, 2020 (1964)Document20 pagesNepal Medical Council Act, 2020 (1964)Madhu Sudhan PandeyaNo ratings yet
- Lecture-11 Breech PresentationDocument27 pagesLecture-11 Breech PresentationMadhu Sudhan PandeyaNo ratings yet
- Teratology & Chronic PoisoningDocument54 pagesTeratology & Chronic PoisoningMadhu Sudhan PandeyaNo ratings yet
- Vaccination Guideline: International Travel and Health 2007Document9 pagesVaccination Guideline: International Travel and Health 2007Madhu Sudhan PandeyaNo ratings yet
- Abortion: Renhe Hospital Wang JunjieDocument51 pagesAbortion: Renhe Hospital Wang JunjieMadhu Sudhan PandeyaNo ratings yet
- Lecture-17 Shoulder DystociaDocument20 pagesLecture-17 Shoulder DystociaMadhu Sudhan PandeyaNo ratings yet
- Lecture-25 Cesarean SectionDocument21 pagesLecture-25 Cesarean SectionMadhu Sudhan PandeyaNo ratings yet
- Lecture-31 Instrumental DeliveryDocument33 pagesLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaNo ratings yet
- Postpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinDocument98 pagesPostpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinMadhu Sudhan Pandeya100% (1)
- Lecture-13 Transeverse LieDocument15 pagesLecture-13 Transeverse LieMadhu Sudhan PandeyaNo ratings yet
- Bishop's Pre-Induction Cervical Scoring SystemDocument2 pagesBishop's Pre-Induction Cervical Scoring SystemMadhu Sudhan PandeyaNo ratings yet
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaNo ratings yet
- Lecture-22 Prolonged PregnancyDocument24 pagesLecture-22 Prolonged PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-26 Hypertensive Disease of PregnancyDocument28 pagesLecture-26 Hypertensive Disease of PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-24 Twins PregnancyDocument30 pagesLecture-24 Twins PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-20 Premature LaborDocument13 pagesLecture-20 Premature LaborMadhu Sudhan PandeyaNo ratings yet
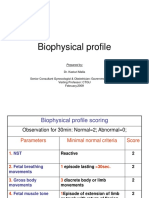
- Lecture-23 Biophysical ProfieDocument3 pagesLecture-23 Biophysical ProfieMadhu Sudhan PandeyaNo ratings yet
- Lecture-12 Face PresentationDocument9 pagesLecture-12 Face PresentationMadhu Sudhan PandeyaNo ratings yet
- Lecture-15 Prolonged LaborDocument8 pagesLecture-15 Prolonged LaborMadhu Sudhan PandeyaNo ratings yet
- Lecture-8 First Stage ManagementDocument10 pagesLecture-8 First Stage ManagementMadhu Sudhan PandeyaNo ratings yet
- Antenatal Care and High Risk PregnancyDocument12 pagesAntenatal Care and High Risk PregnancyMadhu Sudhan PandeyaNo ratings yet
- ICPEbookletDocument24 pagesICPEbookleticpeoregonNo ratings yet
- Clinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingDocument7 pagesClinicopathological Study of Endometrium in Patients With Abnormal Uterine BleedingNazia BhatNo ratings yet
- ProstatectomyDocument9 pagesProstatectomymardsz100% (1)
- Final List of Empanelled Hospitals.1120417Document52 pagesFinal List of Empanelled Hospitals.1120417AkshayKumarNo ratings yet
- Chronic Rhinosinusitis With Nasal Polyps: Clinical PracticeDocument9 pagesChronic Rhinosinusitis With Nasal Polyps: Clinical PracticeAnabel SagasteguiNo ratings yet
- Cancer Control Strategies in NigeriaDocument10 pagesCancer Control Strategies in NigeriaChikezie OnwukweNo ratings yet
- (Pathophysiology of Hemorrhoids) .: RecordsDocument12 pages(Pathophysiology of Hemorrhoids) .: RecordsMaggie CacieNo ratings yet
- Vegetarianism: Sri Swami SivanandaDocument3 pagesVegetarianism: Sri Swami SivanandacusumanofrancNo ratings yet
- Human Anatomy and Physiology 9th Edition Marieb Solutions Manual 1Document11 pagesHuman Anatomy and Physiology 9th Edition Marieb Solutions Manual 1michael100% (45)
- Aiims Institute Day NewsletterDocument99 pagesAiims Institute Day NewsletterAIIMS100% (1)
- Jurnal Home Care 4Document10 pagesJurnal Home Care 4Aida MawaddahNo ratings yet
- Cell InjuryDocument29 pagesCell Injuryማላያላም ማላያላምNo ratings yet
- Bpe, Gramstain, Pap SmearDocument6 pagesBpe, Gramstain, Pap SmearT helper CellsNo ratings yet
- Comparative Study Between Fruit Juice Brand With Special Context of Tropicana and Real in Dehradun City by Mohd Ashad Lovely Professional UniversityDocument84 pagesComparative Study Between Fruit Juice Brand With Special Context of Tropicana and Real in Dehradun City by Mohd Ashad Lovely Professional UniversityAyaz RazaNo ratings yet
- Krylov A 2016Document5 pagesKrylov A 2016Garjita MaesaNo ratings yet
- HazradDocument16 pagesHazradPhan AnNo ratings yet
- Skutki Uboczne W MezoterapiiDocument15 pagesSkutki Uboczne W MezoterapiiSylwia ParkaNo ratings yet
- Klasifikasi Tindakan Bedah Digestif Update 20 Juni 2022 (BPJS)Document7 pagesKlasifikasi Tindakan Bedah Digestif Update 20 Juni 2022 (BPJS)Eko RistiyantoNo ratings yet
- Effects of SmokingDocument4 pagesEffects of SmokingSubodh SonawaneNo ratings yet