You might also like
- Vicki Barr #3 The Hidden Valley MysteryDocument250 pagesVicki Barr #3 The Hidden Valley MysteryPastPresentFuture100% (1)
- Clinical Approach To Isolated Splenomegaly: M M, P M, R KDocument5 pagesClinical Approach To Isolated Splenomegaly: M M, P M, R KlilisNo ratings yet
- 1 s2.0 S0268960X08000787 Main PDFDocument7 pages1 s2.0 S0268960X08000787 Main PDFmohamedhazemelfollNo ratings yet
- Approach To A Child With Pallor and Hepatosplenomegaly: Anirban DasDocument8 pagesApproach To A Child With Pallor and Hepatosplenomegaly: Anirban DasvgmanjunathNo ratings yet
- Hypersplenism: Review Article: November 2012Document12 pagesHypersplenism: Review Article: November 2012V1QT0RNo ratings yet
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDocument5 pagesTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752No ratings yet
- Systemic Disease and The Liver: Maria Isabel Fiel,, Thomas D. SchianoDocument14 pagesSystemic Disease and The Liver: Maria Isabel Fiel,, Thomas D. Schianokhuyennguyenhmu080692No ratings yet
- Hepatomegali in Infant and Children - Pediatrics in Review-2000-Wolf-303-10Document10 pagesHepatomegali in Infant and Children - Pediatrics in Review-2000-Wolf-303-10Reddy LufyanNo ratings yet
- Approach To A Child With Pallor and Hepatosplenomegaly: Anirban Das, MD, DMDocument7 pagesApproach To A Child With Pallor and Hepatosplenomegaly: Anirban Das, MD, DMMarc Lyndon CafinoNo ratings yet
- Lupus NephritisDocument33 pagesLupus NephritisNi MoNo ratings yet
- SpherocytosisDocument4 pagesSpherocytosisMohammed IbrahimNo ratings yet
- Hiperspenisme 2Document6 pagesHiperspenisme 2anakfkubNo ratings yet
- HematuriaDocument42 pagesHematuriaWasim R. IssaNo ratings yet
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399No ratings yet
- SplenomegalyDocument4 pagesSplenomegalydoctorimrankabirNo ratings yet
- Hereditary SpherocytosisDocument23 pagesHereditary SpherocytosisKashan SiddiquiNo ratings yet
- Rapidly Progressive GlomerulonephritisDocument17 pagesRapidly Progressive GlomerulonephritisEasyOrientDNo ratings yet
- Andrade 1979Document7 pagesAndrade 1979Bruno MoraesNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- Hepatomegaly in Neonates and Children: Ann D. Wolf, MD, and Joel E. Lavine, MD, PHDDocument10 pagesHepatomegaly in Neonates and Children: Ann D. Wolf, MD, and Joel E. Lavine, MD, PHDmirfanjee89No ratings yet
- GIT Portal HypertensionDocument24 pagesGIT Portal HypertensionDr.P.NatarajanNo ratings yet
- Isolated Glomerular Disease With Recurrent Gross HematuriaDocument17 pagesIsolated Glomerular Disease With Recurrent Gross HematuriaArun GeorgeNo ratings yet
- Soleimani 2007Document9 pagesSoleimani 2007ceciliaNo ratings yet
- CK SamplesDocument63 pagesCK SamplesAppu ayyala100% (2)
- The Kidneys in Systemic DiseasesDocument65 pagesThe Kidneys in Systemic Diseasesjuanchinn1No ratings yet
- HipersplenismDocument6 pagesHipersplenismDany YayanNo ratings yet
- Diseases of Urinary SystemDocument29 pagesDiseases of Urinary SystemHassan.shehri100% (9)
- Upper Gastrointestinal Endoscopy Is The Diagnostic Study of Choice When A Patient Presents With Acute Alkali Ingestion. 2Document2 pagesUpper Gastrointestinal Endoscopy Is The Diagnostic Study of Choice When A Patient Presents With Acute Alkali Ingestion. 2Mariam MohamedNo ratings yet
- Enfermedad GlomerularDocument7 pagesEnfermedad GlomerularKatty ZanabriaNo ratings yet
- Bazo Errante 2016 REVISED Ijtra1601084Document4 pagesBazo Errante 2016 REVISED Ijtra1601084luisalfredo_montesNo ratings yet
- Spring 2004-05 Final MB Part IIDocument14 pagesSpring 2004-05 Final MB Part IIBen JonesNo ratings yet
- All About Pleural EffusionDocument6 pagesAll About Pleural EffusionTantin KristantoNo ratings yet
- Glomerulonephritis: Lecturer Prof. Yu.R. KovalevDocument39 pagesGlomerulonephritis: Lecturer Prof. Yu.R. Kovalevalfaz lakhani100% (1)
- Radiology Case Report - Splenic AbscessDocument6 pagesRadiology Case Report - Splenic AbscessAbeebNo ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- Liver AbsesDocument8 pagesLiver AbsesS FznsNo ratings yet
- Glomerulonefritis Menbrano Prol N Engl J Med 2012Document13 pagesGlomerulonefritis Menbrano Prol N Engl J Med 2012Francisco Rebollar GarduñoNo ratings yet
- At Two: Was SeDocument3 pagesAt Two: Was Seida ayu agung WijayantiNo ratings yet
- Systemiclupus Erythematosus: Safeandeffective Managementin PrimarycareDocument12 pagesSystemiclupus Erythematosus: Safeandeffective Managementin PrimarycareWilda Dwi FijriyantiNo ratings yet
- Hepatology 04Document7 pagesHepatology 04Fedhi As'adi THearthiefNo ratings yet
- Clinical Features and Diagnosis of Small-Vessel VasculitisDocument13 pagesClinical Features and Diagnosis of Small-Vessel VasculitissigmundmaharajanNo ratings yet
- Case Series of Intussusception in Paediatric SurgeryDocument39 pagesCase Series of Intussusception in Paediatric SurgeryRajkiran AmbarapuNo ratings yet
- Howto Companion August2009Document4 pagesHowto Companion August2009lybrakissNo ratings yet
- Prolonged Fever, Hepatosplenomegaly, and Pancytopenia in A 46-Year-Old WomanDocument6 pagesProlonged Fever, Hepatosplenomegaly, and Pancytopenia in A 46-Year-Old WomanFerdy AlviandoNo ratings yet
- Clinical Approach To RPRF PDFDocument6 pagesClinical Approach To RPRF PDFshankarNo ratings yet
- Mjhid 7 1 E2015036Document3 pagesMjhid 7 1 E2015036Admin neuro-usu.idNo ratings yet
- Case Report PriapismDocument7 pagesCase Report PriapismLaksmi Dewi SaputriNo ratings yet
- Nephrotic Syndrome Msn-3Document12 pagesNephrotic Syndrome Msn-3Bibi Renu100% (3)
- Nephritis LupusDocument8 pagesNephritis LupusDioNo ratings yet
- Set 3 COMP-2Document71 pagesSet 3 COMP-2Appu ayyalaNo ratings yet
- Dob80024 451 458Document8 pagesDob80024 451 458Andreea StreuleaNo ratings yet
- Renal PathologyDocument34 pagesRenal PathologyShanaz ShaxawanNo ratings yet
- GlomerulonephritisDocument4 pagesGlomerulonephritisKim GarciaNo ratings yet
- 77Document6 pages77lilisNo ratings yet
- Liver OneDocument6 pagesLiver Oneeswar6No ratings yet
- Why Does My Patient Limphadenopathy or Splenomegaly?Document14 pagesWhy Does My Patient Limphadenopathy or Splenomegaly?lacmftcNo ratings yet
- Liver Focus 20Document7 pagesLiver Focus 20Sanja CirkovicNo ratings yet
- Choledochal Cyst..Document50 pagesCholedochal Cyst..Ramesh ReddyNo ratings yet
- Capillaria PhilippinenensisDocument4 pagesCapillaria PhilippinenensisnadalabelNo ratings yet
- Contracted PelvisDocument13 pagesContracted PelvisCuteness Romney100% (1)
- Đề 03Document4 pagesĐề 03teachingielts2023No ratings yet
- Ab-Ark Benefit Packages (Private)Document66 pagesAb-Ark Benefit Packages (Private)raamki_99No ratings yet
- Vaccines and SeraDocument19 pagesVaccines and SeraMaulik M Patel100% (1)
- Ieltsfever Academic Reading Practcie Test 50 PDFDocument11 pagesIeltsfever Academic Reading Practcie Test 50 PDFHarman Chandigarhiyaa100% (1)
- Seminar ON HepatitisDocument41 pagesSeminar ON HepatitissomivipinNo ratings yet
- CHN QuestionsDocument10 pagesCHN QuestionsHerne BalberdeNo ratings yet
- Jared Diamond Worst MistakeDocument2 pagesJared Diamond Worst Mistakeapi-190779969No ratings yet
- 1915 Chas M Higgins The Crime Against The School Child PDFDocument72 pages1915 Chas M Higgins The Crime Against The School Child PDFJacek Rafał TatkoNo ratings yet
- Mrunal Pillar 6 Lecture 60-65 @ PDFDocument41 pagesMrunal Pillar 6 Lecture 60-65 @ PDFMd Muneeruddin AhmedNo ratings yet
- ConjunctivaDocument85 pagesConjunctivaMuhammad AboAlasaadNo ratings yet
- Chikungunya Key Facts: TransmissionDocument5 pagesChikungunya Key Facts: TransmissionGlenn L. RavanillaNo ratings yet
- Primary Health Care PHCDocument98 pagesPrimary Health Care PHCDENNIS N. MUÑOZ100% (5)
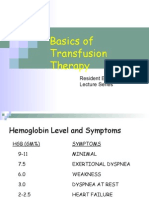
- Basics of Transfusion TherapyDocument43 pagesBasics of Transfusion TherapyMuhammad Afyudin DjumhuriNo ratings yet
- Dr. Rai Muhammad Asghar Associate Professor Pediatrics Head of Pediatric Department RMC RawalpindiDocument34 pagesDr. Rai Muhammad Asghar Associate Professor Pediatrics Head of Pediatric Department RMC RawalpindiHassan AhmadNo ratings yet
- African Swine Fever: Now in WidespreadDocument2 pagesAfrican Swine Fever: Now in WidespreadMariaGlenda Dellosa Guevara-YusonNo ratings yet
- Participatory Rural Appraisal - Report Nov 27thDocument19 pagesParticipatory Rural Appraisal - Report Nov 27thakhilr66No ratings yet
- HepatocytesDocument38 pagesHepatocytesapi-327824087No ratings yet
- Asa PSC System PDFDocument2 pagesAsa PSC System PDFKen WonNo ratings yet
- Tension PneumothoraxDocument9 pagesTension PneumothoraxFadilla Rizki PutriNo ratings yet
- Basics of 5 Element Diagnosis Part X: FLU Prevention AcupunctureDocument15 pagesBasics of 5 Element Diagnosis Part X: FLU Prevention Acupuncturekunfupanda1No ratings yet
- What Are Chemtrails?Document7 pagesWhat Are Chemtrails?Mamello Meme BolofoNo ratings yet
- Maternal Health ProgramDocument5 pagesMaternal Health ProgramMark Kevin Velasco PanchoNo ratings yet
- Opthalmology Image Based QuestionsDocument22 pagesOpthalmology Image Based QuestionsRufus Pietersen Kennedy100% (1)
- ECG Identification QuizDocument40 pagesECG Identification QuizRahul AudenesenNo ratings yet
- 14.PhotoDermDiagnosis Keratotic Papules Over Chest and BackDocument3 pages14.PhotoDermDiagnosis Keratotic Papules Over Chest and BackDwi Tantri SPNo ratings yet
- Рецензия TOEFLDocument2 pagesРецензия TOEFLкатринNo ratings yet
- Dr. Rehab Aljerbi Assistant Lecturer-Department of Family and Community Medicine Tripoli UniversityDocument31 pagesDr. Rehab Aljerbi Assistant Lecturer-Department of Family and Community Medicine Tripoli UniversityHannan AliNo ratings yet