You might also like
- Genetic disorders and recent developments in gene therapyFrom EverandGenetic disorders and recent developments in gene therapyNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Genetic Aneuploidy: Digeorge SyndromeDocument12 pagesGenetic Aneuploidy: Digeorge SyndromeNisha MixonNo ratings yet
- Genetic Aneuploidy: Digeorge SyndromeDocument12 pagesGenetic Aneuploidy: Digeorge SyndromeNisha MixonNo ratings yet
- Direct Immmuno Flourescence Study in Auto Immune Bullous DisordersDocument3 pagesDirect Immmuno Flourescence Study in Auto Immune Bullous DisordersInternational Organization of Scientific Research (IOSR)No ratings yet
- Guillain Barre Syndrome Effects in Child Population PDFDocument4 pagesGuillain Barre Syndrome Effects in Child Population PDFDWI SARAH MAULIDIANo ratings yet
- A Rose Is A Rose Is A Rose But CVID Is Not CVID - Common Variable Immune Deficiency (CVID) What Do We Know in 2011Document61 pagesA Rose Is A Rose Is A Rose But CVID Is Not CVID - Common Variable Immune Deficiency (CVID) What Do We Know in 2011vishnupgiNo ratings yet
- Di GeorgeDocument3 pagesDi Georgethresh mainNo ratings yet
- Di George Syndrome-6 - 1Document6 pagesDi George Syndrome-6 - 1usamas85556No ratings yet
- Digeorge Syndrome Research PaperDocument5 pagesDigeorge Syndrome Research Paperapi-386698528No ratings yet
- Case Study AnalysisDocument3 pagesCase Study AnalysisDominique LopenaNo ratings yet
- Common Variable Immune DeficiencyDocument6 pagesCommon Variable Immune Deficiencyshaf.hybridwhimsyNo ratings yet
- Am J Med Genet C Semin Med Genet 2017 175 516Document8 pagesAm J Med Genet C Semin Med Genet 2017 175 516Biblioteca FleniNo ratings yet
- Bullous Pemphigoid Profile and Outcome in A Series of 100 Cases in SingaporeDocument4 pagesBullous Pemphigoid Profile and Outcome in A Series of 100 Cases in SingaporeJual Beli PromosiNo ratings yet
- DiGeorge Syndrome (DGS)Document11 pagesDiGeorge Syndrome (DGS)Saba Parvin Haque100% (1)
- Digeorge Syndrome: 22q11 DELETIONDocument6 pagesDigeorge Syndrome: 22q11 DELETIONLouie Anne Cardines AnguloNo ratings yet
- Cvid Lancet 2008Document14 pagesCvid Lancet 2008Andre GarciaNo ratings yet
- Brain Awt255Document13 pagesBrain Awt255chsrlyneuro68No ratings yet
- E. DOCK 8 DeficiencyDocument22 pagesE. DOCK 8 DeficiencyAseel AliNo ratings yet
- Hemophagocytic Lymphohistiocytosis in A Child With Chro - 2022 - Medical JournalDocument4 pagesHemophagocytic Lymphohistiocytosis in A Child With Chro - 2022 - Medical JournalAnisha RanaNo ratings yet
- Seminar: Enno Schmidt, Detlef ZillikensDocument13 pagesSeminar: Enno Schmidt, Detlef ZillikensUssiy RachmanNo ratings yet
- Dengue y Esteroides)Document9 pagesDengue y Esteroides)reichell rojasNo ratings yet
- More Than Keratitis, Ichthyosis, and Deafness: Multisystem Effects of Lethal GJB2 MutationsDocument9 pagesMore Than Keratitis, Ichthyosis, and Deafness: Multisystem Effects of Lethal GJB2 MutationsadhastriNo ratings yet
- Soroori-Motlagh Nastaran 200705 (SCID)Document29 pagesSoroori-Motlagh Nastaran 200705 (SCID)Charles IppolitoNo ratings yet
- 7 Rare Cases in IndiaDocument5 pages7 Rare Cases in IndiaNarendran KumaravelNo ratings yet
- Elife 83641 v1Document18 pagesElife 83641 v1PranavNo ratings yet
- Etiology of Proptosis in Children Sindhu 1998Document3 pagesEtiology of Proptosis in Children Sindhu 1998Putri Wulan SukmawatiNo ratings yet
- Chapter 12 Disorders of The Immune Response - UnlockedDocument10 pagesChapter 12 Disorders of The Immune Response - UnlockedThalia FortuneNo ratings yet
- Md3 Quiz: E. T CellsDocument17 pagesMd3 Quiz: E. T CellsBenjamin AgbonzeNo ratings yet
- 1 s2.0 S2049080122003120 MainDocument6 pages1 s2.0 S2049080122003120 MainSalvia Elvaretta HarefaNo ratings yet
- Objective: To Review The Epidemiology, Pathophysiology, and Treatments of Gaucher DiseaseDocument9 pagesObjective: To Review The Epidemiology, Pathophysiology, and Treatments of Gaucher DiseaseShintaAlmayraSaraswatiNo ratings yet
- Version of Record:: ManuscriptDocument7 pagesVersion of Record:: ManuscriptFlavia ChNo ratings yet
- The Various Clinical Spectra of Juvenile Xanthogranuloma: Imaging For Two Case Reports and Review of The LiteratureDocument9 pagesThe Various Clinical Spectra of Juvenile Xanthogranuloma: Imaging For Two Case Reports and Review of The LiteratureAndrés WunderwaldNo ratings yet
- Seminario 2 Inmunologia Clinica 2023-IIDocument9 pagesSeminario 2 Inmunologia Clinica 2023-IImiguel angel ascoy saucedoNo ratings yet
- Sickle Cell Disease DissertationDocument7 pagesSickle Cell Disease DissertationWritingPaperServicesUK100% (1)
- Case Series: Gaucher's Disease: Report of 11 Cases With Review of LiteratureDocument8 pagesCase Series: Gaucher's Disease: Report of 11 Cases With Review of LiteratureNarendran KumaravelNo ratings yet
- Abstract BookDocument90 pagesAbstract BookPopescu RoxanaNo ratings yet
- 2013 Delgado MolSyndromolDocument5 pages2013 Delgado MolSyndromolEAPNo ratings yet
- Congenital Aganglionic Megacolon (Hirschsprung Disease) - UpToDateDocument37 pagesCongenital Aganglionic Megacolon (Hirschsprung Disease) - UpToDateJorge Leonardo BedoyaNo ratings yet
- Surgical Management of Head and Neck RDDDocument6 pagesSurgical Management of Head and Neck RDDDevy OctaviaNo ratings yet
- Cases Journal: A Newborn With Cornelia de Lange Syndrome: A Case ReportDocument5 pagesCases Journal: A Newborn With Cornelia de Lange Syndrome: A Case ReportAyu Wiarni SusanthiNo ratings yet
- Chronic Granulomatous DiseaseDocument2 pagesChronic Granulomatous Diseaseyousrazeidan1979No ratings yet
- cprl1 0708Document3 pagescprl1 0708adlbrlnNo ratings yet
- Advances in Molecular Pathology Into Brain Tumor DiajDocument29 pagesAdvances in Molecular Pathology Into Brain Tumor DiajAkshhata NarulkarNo ratings yet
- Common Variable Immunodeficiency: Epidemiology, Pathogenesis, Clinical Manifestations, Diagnosis, Classification, and ManagementDocument21 pagesCommon Variable Immunodeficiency: Epidemiology, Pathogenesis, Clinical Manifestations, Diagnosis, Classification, and ManagementViviana LunaNo ratings yet
- Research JournalDocument4 pagesResearch JournalHyacinth A RotaNo ratings yet
- General Pathology Bimonthly Exam Compilation Updated 2Document197 pagesGeneral Pathology Bimonthly Exam Compilation Updated 2Cherry Rahima100% (1)
- Introduction To Dendritic Cell Vaccines Immunotherapy For Glioblastoma Multiforme: A Novel ApproachDocument5 pagesIntroduction To Dendritic Cell Vaccines Immunotherapy For Glioblastoma Multiforme: A Novel ApproachparcoxssNo ratings yet
- CaseDocument24 pagesCasecintaNo ratings yet
- Hyperthyroidism in Childhood: Causes, When and How To Treat: ReviewDocument7 pagesHyperthyroidism in Childhood: Causes, When and How To Treat: ReviewSylvia Ruth Alisa NababanNo ratings yet
- Erythema Multiforme/Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis in Lenalidomide-Treated PatientsDocument2 pagesErythema Multiforme/Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis in Lenalidomide-Treated Patientsputu artanaNo ratings yet
- Role of Cat-Scratch Disease in Lymphadenopathy in The Head and NeckDocument7 pagesRole of Cat-Scratch Disease in Lymphadenopathy in The Head and NeckNurizaldo GinusNo ratings yet
- Guillain Barre Syndrome: A Clinical Observational Study in Indian Paediatric PatientsDocument5 pagesGuillain Barre Syndrome: A Clinical Observational Study in Indian Paediatric PatientsLeonardo Antonio Castillo ZegarraNo ratings yet
- DermatomiositisDocument7 pagesDermatomiositisCarlos CalvoNo ratings yet
- 1 s2.0 S2352304219300881 MainDocument12 pages1 s2.0 S2352304219300881 Mainpdfs studiesNo ratings yet
- Ijms 21 05223 PDFDocument42 pagesIjms 21 05223 PDFrohailNo ratings yet
- Trisomy 18 With Multiple Congenital Anomalies A Rare Case Report-3Document4 pagesTrisomy 18 With Multiple Congenital Anomalies A Rare Case Report-3Elna EstherNo ratings yet
- Page From Thompson Thompson Genetics in Medicine 8Document2 pagesPage From Thompson Thompson Genetics in Medicine 8jorgegrodlNo ratings yet
- Challenging Diagnosis of Kimura Disease in A Child With Nephrotic Syndrome: A Case ReportDocument5 pagesChallenging Diagnosis of Kimura Disease in A Child With Nephrotic Syndrome: A Case ReportTalbiya mullaNo ratings yet
- Overview InmunodeficienciaDocument25 pagesOverview InmunodeficienciaLuisa AlandeteNo ratings yet
- Abdomen (Inguinal Hernia) : Anatomy II Block 3 NotesDocument39 pagesAbdomen (Inguinal Hernia) : Anatomy II Block 3 NotesJoseph KimNo ratings yet
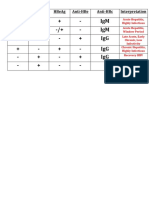
- HBV Antibody InterpretationDocument1 pageHBV Antibody InterpretationJoseph KimNo ratings yet
- First Aid Virology SectionDocument15 pagesFirst Aid Virology SectionJoseph KimNo ratings yet
- CH 18 Cholesterol Metabolism: Biochem Block 3 NotesDocument38 pagesCH 18 Cholesterol Metabolism: Biochem Block 3 NotesJoseph KimNo ratings yet
- Full Notes Embryo DetailedDocument33 pagesFull Notes Embryo DetailedJoseph KimNo ratings yet
- Physio-DES-6 (Cardiac)Document56 pagesPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- Physiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)Document56 pagesPhysiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)Joseph KimNo ratings yet
- Grand Anse To True Blue Weekend Bus 2 Spring 2020Document1 pageGrand Anse To True Blue Weekend Bus 2 Spring 2020Joseph KimNo ratings yet
- Nbme 12 Section 1 AnswersDocument4 pagesNbme 12 Section 1 AnswersDavid LeeNo ratings yet
- Clinical Integration: Lymphatic & Respiratory SystemsDocument13 pagesClinical Integration: Lymphatic & Respiratory SystemsJoseph KimNo ratings yet
- Lymphatic System: Lab Interactive SessionDocument24 pagesLymphatic System: Lab Interactive SessionJoseph KimNo ratings yet
- A True Blue To Grand Anse Master Weekday Spring 2020Document1 pageA True Blue To Grand Anse Master Weekday Spring 2020Joseph KimNo ratings yet
- Respiratory System: Lab Interactive SessionDocument20 pagesRespiratory System: Lab Interactive SessionJoseph KimNo ratings yet
- E True Blue To True Blue Inn Spring 2020Document2 pagesE True Blue To True Blue Inn Spring 2020Joseph KimNo ratings yet
- DiGeorge Case Fall 2016Document3 pagesDiGeorge Case Fall 2016Joseph KimNo ratings yet
- CPR ImcqDocument9 pagesCPR ImcqJoseph KimNo ratings yet
- RNA Viruses ChartDocument1 pageRNA Viruses ChartJoseph KimNo ratings yet
- Virus ClassificationDocument1 pageVirus ClassificationJoseph KimNo ratings yet
- DiGeorge Case Fall 2016 PDFDocument2 pagesDiGeorge Case Fall 2016 PDFJoseph KimNo ratings yet
- VirusesDocument19 pagesVirusesJoseph KimNo ratings yet
- First Aid Virology SectionDocument15 pagesFirst Aid Virology SectionJoseph KimNo ratings yet
- CPR MCQDocument18 pagesCPR MCQJoseph KimNo ratings yet
- Biochemistry DES 9Document47 pagesBiochemistry DES 9Joseph KimNo ratings yet
- CPR MCQDocument11 pagesCPR MCQJoseph KimNo ratings yet
- 02 A Table of Molec Diagnostic Techniques - SP 2016Document4 pages02 A Table of Molec Diagnostic Techniques - SP 2016Joseph KimNo ratings yet
- FoodGroupsAndCaloriesReport DetailedDocument7 pagesFoodGroupsAndCaloriesReport DetailedJoseph KimNo ratings yet
- Physio Lab CasesDocument4 pagesPhysio Lab CasesJoseph KimNo ratings yet
- Mayank Yadav: Academic QualificationDocument2 pagesMayank Yadav: Academic QualificationJacob PruittNo ratings yet
- PGS 504 Notes Part IIDocument3 pagesPGS 504 Notes Part IISejal PriyaNo ratings yet
- Ketone OxidationDocument20 pagesKetone OxidationNgurah MahasviraNo ratings yet
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- SyllabusDocument2 pagesSyllabusPrakash KumarNo ratings yet
- Lab 2 - Capacitive ReactanceDocument4 pagesLab 2 - Capacitive Reactanceali basitNo ratings yet
- Ranitidine + OndansetronDocument7 pagesRanitidine + OndansetronAllicia PutriNo ratings yet
- SAVULESCU, Julian - A Simple Solution To The Puzzles of End of LifeDocument5 pagesSAVULESCU, Julian - A Simple Solution To The Puzzles of End of Lifediradosta_1992No ratings yet
- Arrival Guide To MalaysiaDocument2 pagesArrival Guide To Malaysiaamanu092No ratings yet
- Directory of Acredited Medical Testing LaboratoriesDocument93 pagesDirectory of Acredited Medical Testing LaboratoriesCALIDAD METROMEDICA E.UNo ratings yet
- Paper - Impact of Rapid Urbanization On Agricultural LandsDocument10 pagesPaper - Impact of Rapid Urbanization On Agricultural LandsKosar Jabeen100% (1)
- Pengertian Recount Text Kls 9Document26 pagesPengertian Recount Text Kls 9MARINDRA RETNONo ratings yet
- LinkageDocument47 pagesLinkageTony BernardNo ratings yet
- Anexate IVsolnDocument7 pagesAnexate IVsolnJelena Obrenovic StankovicNo ratings yet
- Multiple Choice Questions: Topic Covered Are As FollowsDocument3 pagesMultiple Choice Questions: Topic Covered Are As FollowsBikash SahuNo ratings yet
- Pressure Regulator FRSDocument6 pagesPressure Regulator FRSTobiasAngererNo ratings yet
- Phaser 3250 Service Manual 0106 2010Document334 pagesPhaser 3250 Service Manual 0106 2010Terry BogardNo ratings yet
- 6 Ijasrjun20196Document8 pages6 Ijasrjun20196TJPRC PublicationsNo ratings yet
- CoC VampireCharacterPrimerPDFDocument5 pagesCoC VampireCharacterPrimerPDFDavid Alexander TomblinNo ratings yet
- HY Endocrine UsmleDocument22 pagesHY Endocrine UsmleNakhal JararNo ratings yet
- SCIENTIFIC BASIS OF HUMAN MOVEMENT EFFECTS OF EXERCISE ON RESPIRATORY SYSTEM - Wbshce PDFDocument9 pagesSCIENTIFIC BASIS OF HUMAN MOVEMENT EFFECTS OF EXERCISE ON RESPIRATORY SYSTEM - Wbshce PDFlancetNo ratings yet
- Is 228 (Part 1) : 1987 Methods For Chemical Analysis Of: (Reaffirmed 2008)Document5 pagesIs 228 (Part 1) : 1987 Methods For Chemical Analysis Of: (Reaffirmed 2008)Indira BanerjeeNo ratings yet
- Type Test Verification SafePlus 12 24 KVDocument8 pagesType Test Verification SafePlus 12 24 KVGary FortuinNo ratings yet
- Spoilage of Frozen Chicken Nuggets by Toxigenic Psycrophilic FungiDocument16 pagesSpoilage of Frozen Chicken Nuggets by Toxigenic Psycrophilic FungiNIDHI BARINo ratings yet
- Fleming Trio-E Promotional SheetDocument2 pagesFleming Trio-E Promotional SheetRed BarnNo ratings yet
- Jeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteDocument2 pagesJeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteCity & State NYNo ratings yet
- Mem CalcDocument6 pagesMem CalcQruisedNo ratings yet
- QTR-2 2023 Meeting Format Nov.23Document45 pagesQTR-2 2023 Meeting Format Nov.23skumar31397No ratings yet
- Case Study NCP ActualDocument3 pagesCase Study NCP Actualdhamy florNo ratings yet