You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- SSA Benefits SummaryDocument2 pagesSSA Benefits SummaryTorgo Thompson0% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Search For TruthDocument64 pagesSearch For TruthJay Cal100% (5)
- Michel Foucault - Two Lectures From Power-KnowledgeDocument6 pagesMichel Foucault - Two Lectures From Power-KnowledgeEzekiel Isa100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Structure of PoetryDocument3 pagesThe Structure of PoetryRose Razo100% (1)
- 2022-02-03 Adidas Global Supplier ListDocument179 pages2022-02-03 Adidas Global Supplier ListTrần Đức Dũng100% (1)
- Sample LetterDocument1 pageSample LetterMohd FadhlyNo ratings yet
- In-Home Supportive Services (Ihss) Program Health Care Certification FormDocument2 pagesIn-Home Supportive Services (Ihss) Program Health Care Certification FormTorgo ThompsonNo ratings yet
- Vanessa Carlton - Devil Dance PDFDocument2 pagesVanessa Carlton - Devil Dance PDFTorgo ThompsonNo ratings yet
- Alanis Morisette - IronicDocument6 pagesAlanis Morisette - IronicSteven RichardAndrewLordNo ratings yet
- How To Trim A Cat's Claws - EdsDocument2 pagesHow To Trim A Cat's Claws - EdsTorgo ThompsonNo ratings yet
- Angelic AlphabetDocument14 pagesAngelic Alphabetgiorgossaridakis100% (6)
- Understanding Rapport and Mind ControlDocument4 pagesUnderstanding Rapport and Mind Controlигнат дълбоковNo ratings yet
- How To Tell If Someone Is LyingDocument1 pageHow To Tell If Someone Is LyingClaudia Burlacu100% (1)
- Derren Brown - Rock Paper ScissorsDocument1 pageDerren Brown - Rock Paper ScissorsklausNo ratings yet
- All About The Hathras Case - IpleadersDocument1 pageAll About The Hathras Case - IpleadersBadhon Chandra SarkarNo ratings yet
- Present Simple and Present Progressive TensesDocument4 pagesPresent Simple and Present Progressive TensesHân NguyễnNo ratings yet
- ADL Report "Attacking" Press TVDocument20 pagesADL Report "Attacking" Press TVGordon DuffNo ratings yet
- Pink Illustrative Weather Quiz Game PresentationDocument28 pagesPink Illustrative Weather Quiz Game PresentationMark Laurenze MangaNo ratings yet
- DocxDocument5 pagesDocxFelicya Angel Ivy LynnNo ratings yet
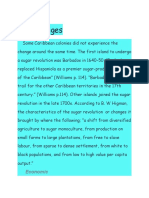
- Effects of The Sugar RevolutionDocument9 pagesEffects of The Sugar RevolutionSusan BarriotNo ratings yet
- B IngDocument2 pagesB IngsyfnanyNo ratings yet
- Society of Radiographers - PDFDocument9 pagesSociety of Radiographers - PDFOsama AhmedNo ratings yet
- Bca SYNOPSISDocument31 pagesBca SYNOPSISjigyasha oarmarNo ratings yet
- Alora Sealord History, How and Why They Were FormedDocument1 pageAlora Sealord History, How and Why They Were Formedgoddessjanefire003No ratings yet
- Financial Management Notes - Dividend Decision - Dynamic Tutorials and ServicesDocument10 pagesFinancial Management Notes - Dividend Decision - Dynamic Tutorials and Servicessimranarora2007No ratings yet
- English DWDM 2022 Book 7 Int Sample PagesDocument7 pagesEnglish DWDM 2022 Book 7 Int Sample PagesLuiz Roberto MartinesNo ratings yet
- 11g SQL Fundamentals I Student Guide - Vol IIDocument283 pages11g SQL Fundamentals I Student Guide - Vol IIIjazKhanNo ratings yet
- Kantar Worldpanel Division FMCG Monitor Q2 2022 EN Including Gift Shared-by-WorldLine-Technology-1Document13 pagesKantar Worldpanel Division FMCG Monitor Q2 2022 EN Including Gift Shared-by-WorldLine-Technology-1K59 Dau Minh VyNo ratings yet
- How To Comp For A Vocalist - Singer - The Jazz Piano SiteDocument5 pagesHow To Comp For A Vocalist - Singer - The Jazz Piano SiteMbolafab RbjNo ratings yet
- Birla Institute of Technology and Science, Pilani: Pilani Campus AUGS/ AGSR DivisionDocument5 pagesBirla Institute of Technology and Science, Pilani: Pilani Campus AUGS/ AGSR DivisionDeep PandyaNo ratings yet
- ITC Gardenia LavendreriaDocument6 pagesITC Gardenia LavendreriaMuskan AgarwalNo ratings yet
- Journeys B2 Teacher's Resource Pack: Grammar ThemesDocument2 pagesJourneys B2 Teacher's Resource Pack: Grammar ThemesMiriam SanchezNo ratings yet
- MAXsys 2510 Meterin FamilyDocument52 pagesMAXsys 2510 Meterin FamilyAbel NinaNo ratings yet
- Curative Petition Draft TutorialDocument4 pagesCurative Petition Draft TutorialBhavya SinghNo ratings yet
- 285519-35126-30-case-studyDocument12 pages285519-35126-30-case-studyapi-737834018No ratings yet
- Faculty of Health and Medical Sciences: Academic Terms and Fee Schedule For 2022Document3 pagesFaculty of Health and Medical Sciences: Academic Terms and Fee Schedule For 2022Sadwi MulatsihNo ratings yet
- Hatch-Slack PathwayDocument10 pagesHatch-Slack Pathwaychurail khanNo ratings yet
- Asian Studies Vol 49 No 2 - 2013Document218 pagesAsian Studies Vol 49 No 2 - 2013Ari Dodol100% (1)
- Final test grammar and vocabulary practiceDocument5 pagesFinal test grammar and vocabulary practicexico_euNo ratings yet
- ANCHETAAADocument79 pagesANCHETAAAGUILAY, KEVIN MARK F.No ratings yet
- Year 11 GCSE Revision Guidance and Exam Booklet Solihull PDFDocument27 pagesYear 11 GCSE Revision Guidance and Exam Booklet Solihull PDFNoor Ulain Nabeela83% (6)