You might also like
- 3 Weeks To A Better Back: Solutions for Healing the Structural, Nutritional, and Emotional Causes of Back PainFrom Everand3 Weeks To A Better Back: Solutions for Healing the Structural, Nutritional, and Emotional Causes of Back PainRating: 4 out of 5 stars4/5 (1)
- A Simple Guide to Pain Management, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pain Management, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Dizziness Questionnaire: When You Are "Dizzy" Do You Experience Any of The Following Symptoms? (Check Yes or No)Document2 pagesDizziness Questionnaire: When You Are "Dizzy" Do You Experience Any of The Following Symptoms? (Check Yes or No)Sudhakar SubramanianNo ratings yet
- VEDA Patient Medical History Form - LongDocument3 pagesVEDA Patient Medical History Form - LongyaddNo ratings yet
- Patient Questionnarie-Dizzinee:vertigoDocument11 pagesPatient Questionnarie-Dizzinee:vertigogulararezendeNo ratings yet
- Chapter 4-ExerciseDocument4 pagesChapter 4-ExerciseWellyNo ratings yet
- Answer Chapter 4-Exercise Sign N SimtomDocument5 pagesAnswer Chapter 4-Exercise Sign N Simtomjessiee yayNo ratings yet
- Islamia College, Peshawar (Icp) Department of Zoology Thyroid Gland Health Assessement QuestionareDocument2 pagesIslamia College, Peshawar (Icp) Department of Zoology Thyroid Gland Health Assessement QuestionareJalil Hijazi AjsNo ratings yet
- Vertigo/Dizziness/Imbalance Questionnaire: Andrew Marlowe, MD, Pa OtolaryngologyDocument2 pagesVertigo/Dizziness/Imbalance Questionnaire: Andrew Marlowe, MD, Pa OtolaryngologyEcaterina ChiriacNo ratings yet
- Vestibular Questionnaire: Fill in The Blank SpacesDocument2 pagesVestibular Questionnaire: Fill in The Blank SpacesyaddNo ratings yet
- Dealing With StressDocument49 pagesDealing With StressMarkee Joyce GalanNo ratings yet
- Health Declaration Form Part A (General) Health Declaration Form Part A (General)Document1 pageHealth Declaration Form Part A (General) Health Declaration Form Part A (General)Jackielou RebualosNo ratings yet
- UNIT II MedicalDocument34 pagesUNIT II Medicalangelax1.1No ratings yet
- Name: Putri Dwi Handayani Reg. No.: P07520117041 Class: 3A Prodi DIII KeperawatanDocument5 pagesName: Putri Dwi Handayani Reg. No.: P07520117041 Class: 3A Prodi DIII KeperawatanPutri Dwi HandayaniNo ratings yet
- Meeting 12 Tugas B Inggris Mita Suci RDocument8 pagesMeeting 12 Tugas B Inggris Mita Suci RMitaNo ratings yet
- Describe Pain New (B.ing)Document4 pagesDescribe Pain New (B.ing)iindearnapurbaNo ratings yet
- Unit 07 Wellbeing - Lesson ADocument45 pagesUnit 07 Wellbeing - Lesson AD inichiNo ratings yet
- Lesson 2 SummaryDocument15 pagesLesson 2 SummarySarah SmithNo ratings yet
- b1b2 Taking Patient History Vocab Questions Worksheet Teachers NotesDocument5 pagesb1b2 Taking Patient History Vocab Questions Worksheet Teachers NotesHakan GünayNo ratings yet
- English II Unit 3.Document9 pagesEnglish II Unit 3.Eddy RodríguezNo ratings yet
- b1b2 Taking Patient History PresentationDocument10 pagesb1b2 Taking Patient History PresentationHakan GünayNo ratings yet
- Staying Healthy: Listening, Reading and Vocabulary ExerciseDocument3 pagesStaying Healthy: Listening, Reading and Vocabulary ExercisevickyNo ratings yet
- New Patient Spine PacketDocument16 pagesNew Patient Spine PacketDebra SmithNo ratings yet
- What Seems To Be The ProblemDocument2 pagesWhat Seems To Be The ProblemJonathan Gomes PiresNo ratings yet
- Height Pass and Vertigo Test Report FormatDocument2 pagesHeight Pass and Vertigo Test Report Formatsyed khaja misbhuddin67% (3)
- Neck Pain Disability QuestionnaireDocument2 pagesNeck Pain Disability QuestionnaireSamuel Iñiguez JiménezNo ratings yet
- Pre-Test: DirectionDocument7 pagesPre-Test: DirectionAhlvaroNo ratings yet
- Nursing Skills ManualDocument52 pagesNursing Skills ManualCamille BattungNo ratings yet
- Regional Write Up Soap Documentation 1 Emily DeskinDocument4 pagesRegional Write Up Soap Documentation 1 Emily Deskinapi-724197922No ratings yet
- 423 Trip To The DoctorDocument2 pages423 Trip To The DoctorAnonymous XsOfDozHauNo ratings yet
- Basico 3Document14 pagesBasico 3Paul Santos IsidroNo ratings yet
- Chương Trình THPT L P 11 - Unit 2Document3 pagesChương Trình THPT L P 11 - Unit 2datuan.workNo ratings yet
- Test AMCUDocument2 pagesTest AMCUSvetlana SolomykinaNo ratings yet
- Grade 7 - Unit 2 - HealthDocument38 pagesGrade 7 - Unit 2 - HealthPhạm Hồng QuyênNo ratings yet
- HA-RLE-WS # 6 Assessing PainDocument3 pagesHA-RLE-WS # 6 Assessing PainJULIE ANNE CORTEZNo ratings yet
- Further Practice Unit 8Document4 pagesFurther Practice Unit 8Uyên HồngNo ratings yet
- Docu 13Document5 pagesDocu 13Kathlyn B. BayranteNo ratings yet
- Taller Maestria 2Document10 pagesTaller Maestria 2Licibeth BetancourthNo ratings yet
- Headache or Migraine, Acute or Chronic?: by Mark ForshawDocument8 pagesHeadache or Migraine, Acute or Chronic?: by Mark ForshawDentisak DokchandraNo ratings yet
- Detailed Lesson Plan in MAPEH Health IIDocument9 pagesDetailed Lesson Plan in MAPEH Health IIMicaela Ongan81% (21)
- CHUVADocument46 pagesCHUVAJUAN MIKHAELNo ratings yet
- Detailed Lesson Plan in MAPEH Health IIDocument8 pagesDetailed Lesson Plan in MAPEH Health IIMa Marisa Arbalate100% (3)
- Unit 3. English II PDFDocument9 pagesUnit 3. English II PDFChrisNo ratings yet
- Week 5 QuestionsDocument2 pagesWeek 5 Questionsapi-502171898No ratings yet
- 2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINDocument5 pages2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINZahirah BudimanNo ratings yet
- Be Review of Systems Questionairet 122714Document1 pageBe Review of Systems Questionairet 122714Djev David DazaNo ratings yet
- Neck Disability IndexDocument1 pageNeck Disability IndexPowChoyNo ratings yet
- The Two Types of Stress AreDocument2 pagesThe Two Types of Stress AreRea Aguilar San PabloNo ratings yet
- PROTOCOL ON PHONOAUDIOLOGICAL ASSESSMENT OF BREATHING WITH SCORING PROPABS Final 03 06 2015Document6 pagesPROTOCOL ON PHONOAUDIOLOGICAL ASSESSMENT OF BREATHING WITH SCORING PROPABS Final 03 06 2015Mariangel CamposNo ratings yet
- Medicine Detail History TakingDocument72 pagesMedicine Detail History TakingqqypprcyxyNo ratings yet
- Unit 10 Health World EnglishDocument25 pagesUnit 10 Health World EnglishFabiola EstradaNo ratings yet
- Unit 2 Health MattersDocument9 pagesUnit 2 Health Matterscarlitamolina2No ratings yet
- TRM SW3 Standard Test U2Document3 pagesTRM SW3 Standard Test U2Mtgarcia PatonNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAhmAd ZuraiDi MahmudNo ratings yet
- Unit 2 Health Lesson 7 Looking Back ProjectDocument50 pagesUnit 2 Health Lesson 7 Looking Back ProjectLê Hương LinhNo ratings yet
- Gordon PDFDocument5 pagesGordon PDFAthena SaturdayNo ratings yet
- Gordons 11 Functional Health PatternsDocument2 pagesGordons 11 Functional Health PatternsCathryn luv QuisidoNo ratings yet
- School Health DeclarationDocument3 pagesSchool Health DeclarationRuchie CardenoNo ratings yet
- Seizure Disorder Case Study ClinicalDocument5 pagesSeizure Disorder Case Study Clinicalapi-546621912No ratings yet
- Mandarin Phrasebook PDFDocument14 pagesMandarin Phrasebook PDFYS Nate0% (1)
- Radio - Mitsubishi Outlander Sport Es 2011 - System Wiring DiagramsDocument7 pagesRadio - Mitsubishi Outlander Sport Es 2011 - System Wiring DiagramsRavi Varakala0% (1)
- POWER SEATS - Mitsubishi Outlander Sport ES 2011 - SYSTEM WIRING DIAGRAMSDocument2 pagesPOWER SEATS - Mitsubishi Outlander Sport ES 2011 - SYSTEM WIRING DIAGRAMSRavi VarakalaNo ratings yet
- GOFLDMTANDB83E1162945588Document2 pagesGOFLDMTANDB83E1162945588Ravi VarakalaNo ratings yet
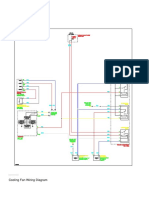
- COOLING FAN - Mitsubishi Outlander Sport ES 2011 - SYSTEM WIRING DIAGRAMSDocument1 pageCOOLING FAN - Mitsubishi Outlander Sport ES 2011 - SYSTEM WIRING DIAGRAMSRavi VarakalaNo ratings yet
- Point and Figure PatternsDocument12 pagesPoint and Figure PatternsRavi VarakalaNo ratings yet
- Mzpack 3 User Guide (En)Document60 pagesMzpack 3 User Guide (En)Ravi Varakala100% (1)
- Coping With Institutional Order Flow Zicklin School of Business Financial Markets SeriesDocument208 pagesCoping With Institutional Order Flow Zicklin School of Business Financial Markets SeriesRavi Varakala100% (5)
- VPA LegendDocument1 pageVPA LegendRavi VarakalaNo ratings yet
- Implied Volatility Excel Sheet.Document1 pageImplied Volatility Excel Sheet.Ravi VarakalaNo ratings yet
- XCEEDDocument12 pagesXCEEDRavi VarakalaNo ratings yet
- BPPV Update Draft Public CommentDocument5 pagesBPPV Update Draft Public CommentRavi VarakalaNo ratings yet
- MAster Candle FB5 Min 27 SLDocument6 pagesMAster Candle FB5 Min 27 SLRavi VarakalaNo ratings yet
- Trade Point GuideDocument400 pagesTrade Point GuideRavi Varakala100% (1)
- Diagnostic Report: Patient Name: Pranav Chauhan PRANM050319990B 0009VA060799Document2 pagesDiagnostic Report: Patient Name: Pranav Chauhan PRANM050319990B 0009VA060799pranav chauhanNo ratings yet
- Vallen AE AccesoriesDocument11 pagesVallen AE AccesoriesSebastian RozoNo ratings yet
- Emergency Floatation Helicoptero PDFDocument14 pagesEmergency Floatation Helicoptero PDFterrywhizardhotmail.com The Best Of The Best.No ratings yet
- Cot 4 Mapeh (Health)Document15 pagesCot 4 Mapeh (Health)RELYN LUCIDONo ratings yet
- File Server Resource ManagerDocument9 pagesFile Server Resource ManagerBùi Đình NhuNo ratings yet
- Compact Switch: Series 96201, 96211, 96221Document2 pagesCompact Switch: Series 96201, 96211, 96221Sales DIGIHU100% (1)
- Btech Me 5 Sem Heat and Mass Transfer Eme504 2020Document2 pagesBtech Me 5 Sem Heat and Mass Transfer Eme504 2020SuryaNo ratings yet
- 311762en WDocument36 pages311762en WOprisor CostinNo ratings yet
- Pre-Qin Philosophers and ThinkersDocument22 pagesPre-Qin Philosophers and ThinkersHelder JorgeNo ratings yet
- Defining The Market Research Problem & Developing An ApproachDocument77 pagesDefining The Market Research Problem & Developing An ApproachSakshi Bhati I H21O41No ratings yet
- TSR 9294 DLA3 Dragons RestDocument78 pagesTSR 9294 DLA3 Dragons RestLéo Duarte100% (4)
- Nursing Care Plan Diabetes Mellitus Type 1Document2 pagesNursing Care Plan Diabetes Mellitus Type 1deric85% (46)
- Water Quality MonitoringDocument3 pagesWater Quality MonitoringJoa YupNo ratings yet
- Forklift Driver Card and Certificate TemplateDocument25 pagesForklift Driver Card and Certificate Templatempac99964% (14)
- Fire and IceDocument11 pagesFire and IcelatishabasilNo ratings yet
- Critical Health Concerns in The 21st CenturyDocument4 pagesCritical Health Concerns in The 21st CenturykelleybrawnNo ratings yet
- 06 Renr5908 08 01 All PDFDocument108 pages06 Renr5908 08 01 All PDFFrancisco Ospino Arrieta100% (2)
- Global Governance and Interstate SystemDocument25 pagesGlobal Governance and Interstate SystemRay Stephen SantosNo ratings yet
- Computer Forensics ReportDocument7 pagesComputer Forensics ReportMatias IacobuzioNo ratings yet
- ECS 3390 - Business and Technical CommuncationsDocument293 pagesECS 3390 - Business and Technical CommuncationsEliseo Robles0% (3)
- Calgary Project Consultants, DubaiDocument18 pagesCalgary Project Consultants, DubaiManish GuptaNo ratings yet
- Module 8 - Facilitating Learner - Centered TeachingDocument4 pagesModule 8 - Facilitating Learner - Centered TeachingSheila Mae Paltep100% (3)
- Tadano450xl PDFDocument12 pagesTadano450xl PDFmunawar0% (1)
- Calculations: M 0 M 1 c1 c1 0 c2 c2 1 2Document6 pagesCalculations: M 0 M 1 c1 c1 0 c2 c2 1 2shadab521100% (1)
- Chapter 7 Integration Testing PDFDocument74 pagesChapter 7 Integration Testing PDFebrgsrtNo ratings yet
- Lesson 3: Letters of RequestDocument4 pagesLesson 3: Letters of RequestMinh HiếuNo ratings yet
- Ask NasaDocument68 pagesAsk Nasacavaco2008No ratings yet
- IBDP Physics Oxford David - Homer Course Ebook 4th Edition-2014 CH-1Document27 pagesIBDP Physics Oxford David - Homer Course Ebook 4th Edition-2014 CH-1Milek Anil KumarNo ratings yet
- Plasterboard FyrchekDocument4 pagesPlasterboard FyrchekAlex ZecevicNo ratings yet
- Holy Spirit Mass SongsDocument57 pagesHoly Spirit Mass SongsRo AnnNo ratings yet