You might also like
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- Vicks Drug of Choice ListDocument17 pagesVicks Drug of Choice Listethank211No ratings yet
- Respi DrugsDocument36 pagesRespi DrugsLady Mae RamosNo ratings yet
- How to Manage Common Digestive IssuesDocument8 pagesHow to Manage Common Digestive IssuesSherlyn BesasNo ratings yet
- NERVOUS MnemonicsDocument4 pagesNERVOUS MnemonicsHimNo ratings yet
- Dams - Last Look - Pharmacology2Document29 pagesDams - Last Look - Pharmacology2skNo ratings yet
- Generic Name Brand Names Common Uses Possible Side Effects Mechanism of ActionDocument13 pagesGeneric Name Brand Names Common Uses Possible Side Effects Mechanism of Actionangel3424No ratings yet
- Vaccination Chart: National Immunization Schedule For New BornDocument20 pagesVaccination Chart: National Immunization Schedule For New BornsmilealwplzNo ratings yet
- Kamal KV 500 Q CollectionsDocument13 pagesKamal KV 500 Q CollectionsBeta ReaderNo ratings yet
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- New Drugs 2019 Mechanisms and UsesDocument6 pagesNew Drugs 2019 Mechanisms and Usesrameez qureshiNo ratings yet
- Pharmacology Questions and AnswersDocument15 pagesPharmacology Questions and AnswersrajuNo ratings yet
- MDS-6-Mock-exam-QAE - Unlocked FINALDocument70 pagesMDS-6-Mock-exam-QAE - Unlocked FINALSubhashNo ratings yet
- Lang 10 EditionDocument235 pagesLang 10 Editionraju niraulaNo ratings yet
- Top 10 Drug InteractionsDocument4 pagesTop 10 Drug InteractionsLeyla MajundaNo ratings yet
- Primary Care Perspective on Pediatric HeadachesDocument34 pagesPrimary Care Perspective on Pediatric HeadachesVirda Maharani100% (2)
- Low Iron DiagnosisDocument12 pagesLow Iron DiagnosisAlexandra RenneNo ratings yet
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinNo ratings yet
- Oral Cases Study Guide - PediatricsDocument68 pagesOral Cases Study Guide - PediatricsJohn100% (1)
- Mishba +pharmacology + Tapan ShahDocument232 pagesMishba +pharmacology + Tapan ShahRaushan BlakeNo ratings yet
- DRUG ALLERGY GUIDEDocument61 pagesDRUG ALLERGY GUIDEadysti100% (1)
- 19 Subjects Imp TopicsDocument24 pages19 Subjects Imp TopicsVenkatesh KS 233100% (1)
- Consensus guidelines for treatment of pediatric nephrotic syndromeDocument14 pagesConsensus guidelines for treatment of pediatric nephrotic syndromeSara Ilyas KhanNo ratings yet
- Ministry of Health and Child Care: Pharmacognosy 28 January 2020Document7 pagesMinistry of Health and Child Care: Pharmacognosy 28 January 2020Von Valentine MhuteNo ratings yet
- The clinical value of blood testsDocument35 pagesThe clinical value of blood testsAgus SyaifudinNo ratings yet
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Drug of Choice and DiseasesDocument2 pagesDrug of Choice and DiseasesJamesNo ratings yet
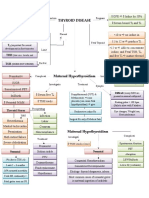
- Thyroid DiseaseDocument1 pageThyroid DiseaseZiyadNo ratings yet
- FMGE July 2023 PrepLadder 1Document558 pagesFMGE July 2023 PrepLadder 1Sahil AhlawatNo ratings yet
- NORADRENALINE (Norepinephrine) : Presentation DescriptionDocument3 pagesNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraNo ratings yet
- Drugs of ChoiceDocument1 pageDrugs of ChoiceMontu ChakmaNo ratings yet
- Approach to Dyslipidemia Based on 2015 CPGDocument26 pagesApproach to Dyslipidemia Based on 2015 CPGRenzy SalumbreNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- GSDDocument26 pagesGSDFahad Ali NadeemNo ratings yet
- A To Z Diseases LISTS For NEETPGDocument5 pagesA To Z Diseases LISTS For NEETPGQworldNo ratings yet
- Review Handouts For Medical Pharmacology PDFDocument21 pagesReview Handouts For Medical Pharmacology PDFAndres F. TorresNo ratings yet
- Antibiotics 9Document11 pagesAntibiotics 9Beth Morales100% (1)
- Epilepsy: Causes of Seizures (Non-Epileptic)Document5 pagesEpilepsy: Causes of Seizures (Non-Epileptic)humdingerNo ratings yet
- Autacoids For Med.Document140 pagesAutacoids For Med.Feysal AhmedNo ratings yet
- Pharmacology 2 Long Exam Oncology-NkDocument7 pagesPharmacology 2 Long Exam Oncology-NkT'amo HanashNo ratings yet
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocument8 pagesApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuNo ratings yet
- Pharmacology Exam4 ReviewDocument8 pagesPharmacology Exam4 ReviewNatalia BortellNo ratings yet
- Basic Pharmacology OverviewDocument42 pagesBasic Pharmacology OverviewWin Htet0% (1)
- Pharma LMRP 2019Document30 pagesPharma LMRP 2019sk100% (1)
- Drugs of Choice for CNS, Blood, GIT, Endo & Chemo /TITLEDocument9 pagesDrugs of Choice for CNS, Blood, GIT, Endo & Chemo /TITLESHAKEEL1991No ratings yet
- CANCER CHEMOTHERAPY REGIMENS AND THEIR TOXICITIESDocument13 pagesCANCER CHEMOTHERAPY REGIMENS AND THEIR TOXICITIESVaibhav Bharat100% (1)
- Antidotes To Common PoisonsDocument5 pagesAntidotes To Common PoisonsAnusha VergheseNo ratings yet
- Essential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 2 PDFDocument1 pageEssential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 2 PDFMariam Qais100% (1)
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- Drug ClassDocument13 pagesDrug ClassEdfren Salazar Colon100% (1)
- Whole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsDocument17 pagesWhole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsFlorina TrutescuNo ratings yet
- Memorize Common Drug Side EffectsDocument2 pagesMemorize Common Drug Side EffectsAngelic khanNo ratings yet
- Mechanism of Action For Each Class of AntiDocument146 pagesMechanism of Action For Each Class of AntiReynaldo RiveraNo ratings yet
- Antibiotic GuideDocument6 pagesAntibiotic GuideAnnTran100% (1)
- Transplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014Document54 pagesTransplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014AbiNo ratings yet
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- Implementation of Hospital Health Promotion at Airlangga University Hospital SurabayaDocument15 pagesImplementation of Hospital Health Promotion at Airlangga University Hospital SurabayaMala OktavianiNo ratings yet
- 2017 ACC AHA VASCD Slide SetDocument96 pages2017 ACC AHA VASCD Slide SetMuhd Nico DariyantoNo ratings yet
- Small Engines CH 1Document13 pagesSmall Engines CH 1shrivdNo ratings yet
- Pharma CollectionDocument40 pagesPharma CollectionMuhd Nico DariyantoNo ratings yet
- Announcement Chest 2019Document4 pagesAnnouncement Chest 2019Muhd Nico DariyantoNo ratings yet
- Anti Retro Viral TherapyDocument156 pagesAnti Retro Viral TherapyMubiru Sylvia100% (2)
- ThyroidDocument16 pagesThyroidnawaNo ratings yet
- Anti Retro Viral TherapyDocument156 pagesAnti Retro Viral TherapyMubiru Sylvia100% (2)
- ThyroidDocument16 pagesThyroidnawaNo ratings yet
- LLLDocument2 pagesLLLrii bundaarifNo ratings yet
- LLLDocument2 pagesLLLrii bundaarifNo ratings yet
- Pharma KatzungDocument22 pagesPharma KatzungMaida PootNo ratings yet
- Anti CholinergicsDocument25 pagesAnti Cholinergicsshahid kNo ratings yet
- 2 - AnsDocument21 pages2 - Ansyahomed519No ratings yet
- Neuropharmacology 1Document15 pagesNeuropharmacology 1Pranjali WeladiNo ratings yet
- Rumpler MDocument218 pagesRumpler Mlucas ronieryNo ratings yet
- Pharmacology of Autonomic Nervous System 2013Document166 pagesPharmacology of Autonomic Nervous System 2013Adimera TsehayeNo ratings yet
- 1st Generation Anti-HistaminesDocument3 pages1st Generation Anti-HistaminesspringdingNo ratings yet
- Pharmacology Test 1 Drug ListDocument20 pagesPharmacology Test 1 Drug ListSHRIKANTNo ratings yet
- Anticholinergic DrugsDocument19 pagesAnticholinergic DrugseashshankarNo ratings yet
- A35. Autonomic Nervous System PharmacologyDocument18 pagesA35. Autonomic Nervous System PharmacologyThư PhạmNo ratings yet
- Questions About PharmacologyDocument83 pagesQuestions About PharmacologyHomman TommanNo ratings yet
- Cholinergic AntagonistsDocument18 pagesCholinergic AntagonistsApurba Sarker Apu100% (1)
- PHARMACOLOGYDocument21 pagesPHARMACOLOGYAllisson BeckersNo ratings yet
- Anticholinergic SDocument22 pagesAnticholinergic SALNAKINo ratings yet
- BLOK 12 - IT 5 - Obat Otonom Antikolinergik - MTKDocument58 pagesBLOK 12 - IT 5 - Obat Otonom Antikolinergik - MTKtattosssNo ratings yet
- Chapter 8. Cholinoceptor Blockers & Amp Cholinesterase RegeneratorsDocument8 pagesChapter 8. Cholinoceptor Blockers & Amp Cholinesterase RegeneratorsChrysler Hans GuttenbergNo ratings yet
- Global Initiative For Chronic Obstructive Lung DiseaseDocument27 pagesGlobal Initiative For Chronic Obstructive Lung DiseaseAla'a MustafaNo ratings yet
- PHC 513: Pharmacology of Drugs Affecting the Peripheral Nervous SystemDocument19 pagesPHC 513: Pharmacology of Drugs Affecting the Peripheral Nervous SystemAimanRozlanNo ratings yet
- Active Ingredients Drug Classification EgyptDocument61 pagesActive Ingredients Drug Classification EgyptBassem WolselyNo ratings yet
- Cholinoceptor AntagonistDocument21 pagesCholinoceptor Antagonistraafat mohammedNo ratings yet
- Seminar On Chronic Obstructive Pulmonary Disease (Copd)Document40 pagesSeminar On Chronic Obstructive Pulmonary Disease (Copd)Soniya Nakka100% (1)
- Orgmed-1 2019Document165 pagesOrgmed-1 2019Joslin Roz GalileaNo ratings yet
- (CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaDocument41 pages(CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaRahman Anwar100% (1)
- Terriann Crisp Usmle Step 1 Pharmacology Review Flash 2014Document330 pagesTerriann Crisp Usmle Step 1 Pharmacology Review Flash 2014Churschmann Spiral100% (3)
- IVMS Pharmacology Flash FactsDocument8,250 pagesIVMS Pharmacology Flash FactsMarc Imhotep Cray, M.D.No ratings yet
- Hypersalivation - What Drug Treatment Options Are Available?Document5 pagesHypersalivation - What Drug Treatment Options Are Available?Kanwal NafisNo ratings yet
- Anticholinergic Drugs: Atropine, Scopolamine, GlycopyrrolateDocument7 pagesAnticholinergic Drugs: Atropine, Scopolamine, GlycopyrrolateLourdes RamírezNo ratings yet
- Cholinergic BlockersDocument39 pagesCholinergic BlockersAmanuel MaruNo ratings yet
- Pharmacology Test 1Document39 pagesPharmacology Test 1Niki BolinNo ratings yet
- 09 Muscarinic Antagonists (Notes - Q A) AtfDocument1 page09 Muscarinic Antagonists (Notes - Q A) Atfaasingh7800No ratings yet