You might also like
- Health informatics: Improving patient careFrom EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITRating: 3 out of 5 stars3/5 (1)
- Acceptability of Information Technology Systems Developed For Distant Philippine Communitiesamong Local Health ProvidersDocument8 pagesAcceptability of Information Technology Systems Developed For Distant Philippine Communitiesamong Local Health ProvidersAr-jay PorrasNo ratings yet
- Peter Fleming, NEHTA, The Future Is Now - Electronic Health in AustraliaDocument21 pagesPeter Fleming, NEHTA, The Future Is Now - Electronic Health in AustraliaDepartment of Broadband, Communications and the Digital EconomyNo ratings yet
- Emental Health 2020 Vision and Strategy For AustraliaDocument12 pagesEmental Health 2020 Vision and Strategy For AustraliaAn MartínezNo ratings yet
- Acceptabilityof ITSystemsfor Distant Health ProvidersDocument9 pagesAcceptabilityof ITSystemsfor Distant Health Providersdumperacct123No ratings yet
- Week 1Document24 pagesWeek 1AfNo ratings yet
- Nursing Tics in EuropeDocument12 pagesNursing Tics in EuropeLiezl Mae MacaraegNo ratings yet
- The State of Telehealth and Telecare in The UK: Prospects For Integrated CareDocument8 pagesThe State of Telehealth and Telecare in The UK: Prospects For Integrated CareAlejandro CardonaNo ratings yet
- 5 Informatics and HealthcareDocument32 pages5 Informatics and HealthcareKyla OnaNo ratings yet
- Chapter 9.a New TechnologiesDocument9 pagesChapter 9.a New TechnologieslaniNo ratings yet
- Integration Context NRHMDocument34 pagesIntegration Context NRHMSanchita MondalNo ratings yet
- Module 14Document5 pagesModule 14camille nina jane navarroNo ratings yet
- Final Project - Limitations of TelehealthDocument13 pagesFinal Project - Limitations of TelehealthPriyanka TanwarNo ratings yet
- New Technologies Related To Public Health Electronic InformationDocument22 pagesNew Technologies Related To Public Health Electronic InformationKhams TolentinoNo ratings yet
- Brief 4Document2 pagesBrief 4raffickbowen2731No ratings yet
- Philippine Health Delivery SystemDocument9 pagesPhilippine Health Delivery SystemMichael Philip CervantesNo ratings yet
- Introduction-Accrediting AgenciesDocument6 pagesIntroduction-Accrediting AgenciesFersan AngelesNo ratings yet
- CU Week 16 New Technologies Related To Public Health Electronic InformationdocxDocument13 pagesCU Week 16 New Technologies Related To Public Health Electronic Informationdocxarmanuel1390antNo ratings yet
- Benefits OfTelemedicineDocument6 pagesBenefits OfTelemedicineMurangwa AlbertNo ratings yet
- Tizon, R. - Assignment in NCM 112Document4 pagesTizon, R. - Assignment in NCM 112Royce Vincent TizonNo ratings yet
- Healthcare and TechnologyDocument16 pagesHealthcare and TechnologyAlan MudaryNo ratings yet
- Final Topic Ehealth MODULE 1Document8 pagesFinal Topic Ehealth MODULE 1folkloriantaroNo ratings yet
- Curs 14Document16 pagesCurs 14cata86_mailNo ratings yet
- International PerspectivesDocument52 pagesInternational PerspectivesAnjo Pasiolco Canicosa100% (1)
- Concept Note of The Primary Health Care QOC ActivityDocument21 pagesConcept Note of The Primary Health Care QOC ActivityTewodros Worku LiyewNo ratings yet
- RA 11223 + F1 For HealthDocument3 pagesRA 11223 + F1 For HealthdeevoncNo ratings yet
- Tizon, R. - Assignment in NCM 112Document4 pagesTizon, R. - Assignment in NCM 112Royce Vincent TizonNo ratings yet
- Using ICT in SchoolDocument5 pagesUsing ICT in Schoolsiti syuhada binti zainalNo ratings yet
- Lesson 4-Overview of Health InformaticsDocument22 pagesLesson 4-Overview of Health InformaticsGHEIST INC.No ratings yet
- Ehealth in The Community Setting: Organization, 2012)Document4 pagesEhealth in The Community Setting: Organization, 2012)Mary Dale Omanea Almodal100% (1)
- Telemedicine: Telehealth vs. Telemedicine What Is ? DisavantagesDocument49 pagesTelemedicine: Telehealth vs. Telemedicine What Is ? DisavantagesERIKA ANNE CADAWANNo ratings yet
- Tech For Patient SafetyDocument66 pagesTech For Patient SafetymasyitahNo ratings yet
- Module 3 TelemedicineDocument15 pagesModule 3 TelemedicineSanath ChowkiNo ratings yet
- New Technologies On Public Health: Dr. Judith J. Sugay Faculty, Feu-InDocument23 pagesNew Technologies On Public Health: Dr. Judith J. Sugay Faculty, Feu-InBianca SandovalNo ratings yet
- PWC Case Study 2021Document7 pagesPWC Case Study 2021Anna PrasitdamrongNo ratings yet
- For Sir Jerry ZorillaDocument10 pagesFor Sir Jerry ZorillaWilma EstebanNo ratings yet
- PAHOIMSEIHCOVID-19200029A EngDocument4 pagesPAHOIMSEIHCOVID-19200029A Engfisioterapi 2019No ratings yet
- IT Governance: A Simple Solution To The Complex Problem of Building National Scale Health Information SystemsDocument34 pagesIT Governance: A Simple Solution To The Complex Problem of Building National Scale Health Information SystemsRico EdureseNo ratings yet
- Information Technology Will Save Health Care: Institute of MedicineDocument7 pagesInformation Technology Will Save Health Care: Institute of MedicineKelvin Kurt B. AgwilangNo ratings yet
- Telehealth Research and Evaluation Implications For Decision MakersDocument9 pagesTelehealth Research and Evaluation Implications For Decision Makerscharlsandroid01No ratings yet
- Western New York Beacon CommunityDocument3 pagesWestern New York Beacon CommunityONC for Health Information TechnologyNo ratings yet
- SCP 2013 2014 Web en Jan 21Document4 pagesSCP 2013 2014 Web en Jan 21Scott PooleNo ratings yet
- Unsolicited Business ProposalDocument6 pagesUnsolicited Business ProposalBengielyn DanaoNo ratings yet
- Telepsychiatry in The 21 Century: Transforming Healthcare With TechnologyDocument17 pagesTelepsychiatry in The 21 Century: Transforming Healthcare With TechnologyEngr Gaddafi Kabiru MarafaNo ratings yet
- Dossier Presentation v01Document7 pagesDossier Presentation v01nikheltauraniNo ratings yet
- Summary of HISDocument7 pagesSummary of HISGNo ratings yet
- Building Blocks of Healthcare SystemDocument9 pagesBuilding Blocks of Healthcare SystemSamantha CorpuzNo ratings yet
- Trends Affecting NSG PracticeDocument22 pagesTrends Affecting NSG PracticeshaitabliganNo ratings yet
- Assignment 1, Semester 1Document9 pagesAssignment 1, Semester 1Notch Melvin MabundaNo ratings yet
- Types of TelemedicinesDocument6 pagesTypes of TelemedicinesRahul BhagatNo ratings yet
- Chapter OneDocument29 pagesChapter OneAbebe ChekolNo ratings yet
- 1.0 Background of The StudyDocument15 pages1.0 Background of The StudyAmrutha PrakashNo ratings yet
- DOH Manual of Standards For Primary Care Facilities (Philippines, 13apr2020)Document52 pagesDOH Manual of Standards For Primary Care Facilities (Philippines, 13apr2020)Jason Suquila100% (2)
- M6 C. E-Health Situation in The PhilippinesDocument10 pagesM6 C. E-Health Situation in The PhilippinesKoleen Lhyte UyNo ratings yet
- Final Position PaperDocument2 pagesFinal Position PaperPRANAVHESH MoeNo ratings yet
- PH Community PlatformDocument5 pagesPH Community PlatformMohd Nor Faizal ZulkifliNo ratings yet
- AYUSHMAN BHARAT - Lec 7th SemDocument61 pagesAYUSHMAN BHARAT - Lec 7th SempriyankaNo ratings yet
- 3208-Article Text-41467-2-10-20211203Document12 pages3208-Article Text-41467-2-10-20211203Nathan MielNo ratings yet
- Information Technology in MedicineDocument13 pagesInformation Technology in MedicineJake MillerNo ratings yet
- FINALS ReviewerDocument14 pagesFINALS ReviewerJustine Simeon lagunzadNo ratings yet
- Brand Descriptions: Abercrombie & Fitch (A & F)Document17 pagesBrand Descriptions: Abercrombie & Fitch (A & F)Suryansh SinghNo ratings yet
- Assessed The Impact of The Corona Crisis On Sponsorships in Sports and Agriculture Industry in IndiaDocument1 pageAssessed The Impact of The Corona Crisis On Sponsorships in Sports and Agriculture Industry in IndiaSuryansh SinghNo ratings yet
- Price XiaomiDocument6 pagesPrice XiaomiSuryansh SinghNo ratings yet
- DIENA Case SolutionDocument8 pagesDIENA Case SolutionSuryansh SinghNo ratings yet
- Name of The Examination Ammount Result: Qualified Qualified QualifiedDocument2 pagesName of The Examination Ammount Result: Qualified Qualified QualifiedSuryansh SinghNo ratings yet
- AignmentDocument3 pagesAignmentSuryansh SinghNo ratings yet
- Brand Name Website LinkDocument3 pagesBrand Name Website LinkSuryansh SinghNo ratings yet
- IDirect FMCG SectorUpdate Mar20 PDFDocument9 pagesIDirect FMCG SectorUpdate Mar20 PDFSuryansh SinghNo ratings yet
- Result Writeup Latest 15112019Document22 pagesResult Writeup Latest 15112019Suryansh SinghNo ratings yet
- Plag Check 1Document2 pagesPlag Check 1Suryansh SinghNo ratings yet
- Financial Savings InfosysDocument2 pagesFinancial Savings InfosysSuryansh SinghNo ratings yet
- Contactless DemonstrationDocument1 pageContactless DemonstrationSuryansh SinghNo ratings yet
- IDirect Auto SectorUpdate 27mar20 PDFDocument13 pagesIDirect Auto SectorUpdate 27mar20 PDFSuryansh SinghNo ratings yet
- IDirect OilGas SectorUpdate Mar20 PDFDocument12 pagesIDirect OilGas SectorUpdate Mar20 PDFSuryansh SinghNo ratings yet
- Bharat Petroleum Corporation: Recovery in Demand Key To Profitability..Document8 pagesBharat Petroleum Corporation: Recovery in Demand Key To Profitability..Suryansh SinghNo ratings yet
- IM ValueAnalysisDocument1 pageIM ValueAnalysisSuryansh SinghNo ratings yet
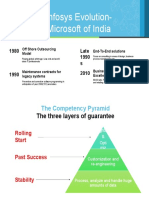
- Infosys Evolution-Microsoft of India: 1980 Late 1990 S 1990 2010Document2 pagesInfosys Evolution-Microsoft of India: 1980 Late 1990 S 1990 2010Suryansh SinghNo ratings yet
- Infosys: Growing Share of Customer Business: Group 1Document8 pagesInfosys: Growing Share of Customer Business: Group 1Suryansh SinghNo ratings yet
- Industrial Marketing: Infosys Technologies LTD.: Growing Share of A Customer's BusinessDocument8 pagesIndustrial Marketing: Infosys Technologies LTD.: Growing Share of A Customer's BusinessSuryansh SinghNo ratings yet
- CSR Initiatives Related To Procurement and Suppliers: Organic CottonDocument2 pagesCSR Initiatives Related To Procurement and Suppliers: Organic CottonSuryansh SinghNo ratings yet
- Uts Chapter 1 Lesson 4Document7 pagesUts Chapter 1 Lesson 4John Jerome GironellaNo ratings yet
- Coaching Fidelity Checklist Intervention 4Document6 pagesCoaching Fidelity Checklist Intervention 4api-438626249No ratings yet
- Proposal On "Design Guidelines For Urban Housing at Dharans Sub Metropolitancity"Document37 pagesProposal On "Design Guidelines For Urban Housing at Dharans Sub Metropolitancity"Prajina ShresthaNo ratings yet
- "Section 1. Any Person or Persons Who Shall Commit Estafa or Other Forms of Swindling AsDocument4 pages"Section 1. Any Person or Persons Who Shall Commit Estafa or Other Forms of Swindling AskaiNo ratings yet
- President Donald J. Trump's Accomplishment List Archive. - MAGAPILL PDFDocument33 pagesPresident Donald J. Trump's Accomplishment List Archive. - MAGAPILL PDFpeter100% (1)
- Siop PPDocument1 pageSiop PPapi-565608712No ratings yet
- Formal and Informal Register Part 2Document3 pagesFormal and Informal Register Part 2Ignacio NoriaNo ratings yet
- Postcolonialism... Involves A Studied Engagement With The Experience of Colonialism and Its Past and Present EffectsDocument3 pagesPostcolonialism... Involves A Studied Engagement With The Experience of Colonialism and Its Past and Present EffectsParimal K SinghNo ratings yet
- Gen Ed 6 Art Appreciation Part1. Multiple Choice (15 Items)Document5 pagesGen Ed 6 Art Appreciation Part1. Multiple Choice (15 Items)Kathleen FamilarNo ratings yet
- Bioethics Module For GE EthicsDocument11 pagesBioethics Module For GE EthicsErrol BuenaventuraNo ratings yet
- MGT617Document14 pagesMGT617Youtube Theater100% (2)
- Ecospace KolkataDocument2 pagesEcospace Kolkataruchithareja50% (2)
- Labor Case Digest Part 2Document35 pagesLabor Case Digest Part 2Trix BermosaNo ratings yet
- Deficiency of Basic Life SkillsDocument1 pageDeficiency of Basic Life SkillsTrần Quỳnh TrangNo ratings yet
- 3-The Herrmann Thinking Styles Model PDFDocument13 pages3-The Herrmann Thinking Styles Model PDFTu TranNo ratings yet
- Job Hopping VS Employee LoyaltyDocument4 pagesJob Hopping VS Employee LoyaltyIffah ImaninaNo ratings yet
- Capstone Group: Global Blockchain ConsultingDocument22 pagesCapstone Group: Global Blockchain ConsultingdigmesNo ratings yet
- Automation PDFDocument2 pagesAutomation PDFNiranjan SalunkeNo ratings yet
- Accreditation of Construction Workers2Document2 pagesAccreditation of Construction Workers2IdrisNo ratings yet
- Oregon Inmate Search Department of Corrections LookupDocument6 pagesOregon Inmate Search Department of Corrections Lookupinmatesearchinfo0% (1)
- Value AnalysisDocument5 pagesValue AnalysisYAqoob DesaiNo ratings yet
- Final Exam 605Document3 pagesFinal Exam 605Franchesca Vargas100% (7)
- Session Plan Mine 1Document79 pagesSession Plan Mine 1Ceniza Del Rosario LopezNo ratings yet
- Questionnaire For Employee Reward and RecognitionDocument7 pagesQuestionnaire For Employee Reward and RecognitionPridhivraj NaiduNo ratings yet
- Tourism in Transitions: Dieter K. Müller Marek Więckowski EditorsDocument212 pagesTourism in Transitions: Dieter K. Müller Marek Więckowski EditorsraisincookiesNo ratings yet
- Sodus CSD Re-Opening PlanDocument41 pagesSodus CSD Re-Opening PlanNews 8 WROCNo ratings yet
- IPR Workshop - Biotech and PharmaDocument9 pagesIPR Workshop - Biotech and PharmaCheshta SharmaNo ratings yet
- The Preparedness of Pre-Service Teachers On The Required Programs To Meet StandardsDocument18 pagesThe Preparedness of Pre-Service Teachers On The Required Programs To Meet StandardsGlobal Research and Development Services100% (1)
- Application Form For The Mofa Taiwan ScholarshipDocument8 pagesApplication Form For The Mofa Taiwan ScholarshipLucien BernardNo ratings yet
- Gisele ResumeDocument5 pagesGisele Resumeapi-462257026No ratings yet
- Chaos Monkeys: Obscene Fortune and Random Failure in Silicon ValleyFrom EverandChaos Monkeys: Obscene Fortune and Random Failure in Silicon ValleyRating: 3.5 out of 5 stars3.5/5 (111)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Cyber War: The Next Threat to National Security and What to Do About ItFrom EverandCyber War: The Next Threat to National Security and What to Do About ItRating: 3.5 out of 5 stars3.5/5 (66)
- Learn Python Programming for Beginners: Best Step-by-Step Guide for Coding with Python, Great for Kids and Adults. Includes Practical Exercises on Data Analysis, Machine Learning and More.From EverandLearn Python Programming for Beginners: Best Step-by-Step Guide for Coding with Python, Great for Kids and Adults. Includes Practical Exercises on Data Analysis, Machine Learning and More.Rating: 5 out of 5 stars5/5 (34)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- Scary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldFrom EverandScary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldRating: 4.5 out of 5 stars4.5/5 (55)
- AP Computer Science A Premium, 2024: 6 Practice Tests + Comprehensive Review + Online PracticeFrom EverandAP Computer Science A Premium, 2024: 6 Practice Tests + Comprehensive Review + Online PracticeNo ratings yet
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Generative AI: The Insights You Need from Harvard Business ReviewFrom EverandGenerative AI: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (2)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- ChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindFrom EverandChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindNo ratings yet
- Chip War: The Quest to Dominate the World's Most Critical TechnologyFrom EverandChip War: The Quest to Dominate the World's Most Critical TechnologyRating: 4.5 out of 5 stars4.5/5 (229)
- CompTIA Security+ Get Certified Get Ahead: SY0-701 Study GuideFrom EverandCompTIA Security+ Get Certified Get Ahead: SY0-701 Study GuideRating: 5 out of 5 stars5/5 (2)
- Excel Essentials: A Step-by-Step Guide with Pictures for Absolute Beginners to Master the Basics and Start Using Excel with ConfidenceFrom EverandExcel Essentials: A Step-by-Step Guide with Pictures for Absolute Beginners to Master the Basics and Start Using Excel with ConfidenceNo ratings yet
- Working with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)From EverandWorking with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)Rating: 5 out of 5 stars5/5 (5)
- The Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldFrom EverandThe Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldRating: 4.5 out of 5 stars4.5/5 (107)
- Four Battlegrounds: Power in the Age of Artificial IntelligenceFrom EverandFour Battlegrounds: Power in the Age of Artificial IntelligenceRating: 5 out of 5 stars5/5 (5)
- Sweet Spot UX: Communicating User Experience to Stakeholders, Decision Makers and Other HumansFrom EverandSweet Spot UX: Communicating User Experience to Stakeholders, Decision Makers and Other HumansRating: 4.5 out of 5 stars4.5/5 (5)
- Understanding Software: Max Kanat-Alexander on simplicity, coding, and how to suck less as a programmerFrom EverandUnderstanding Software: Max Kanat-Alexander on simplicity, coding, and how to suck less as a programmerRating: 4.5 out of 5 stars4.5/5 (44)
- 100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziFrom Everand100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziNo ratings yet
- Solutions Architect's Handbook: Kick-start your career as a solutions architect by learning architecture design principles and strategiesFrom EverandSolutions Architect's Handbook: Kick-start your career as a solutions architect by learning architecture design principles and strategiesNo ratings yet