You might also like
- Devastating Nuclear Accidents throughout History: Causes and Results - Science Book for Kids 9-12 | Children's Science & Nature BooksFrom EverandDevastating Nuclear Accidents throughout History: Causes and Results - Science Book for Kids 9-12 | Children's Science & Nature BooksNo ratings yet
- Case Study: Space Shuttle Challenger DisasterDocument18 pagesCase Study: Space Shuttle Challenger DisasterPorkavi GNo ratings yet
- Three Mile Island Nuclear Accident of 1979Document22 pagesThree Mile Island Nuclear Accident of 1979VP Ch4nelNo ratings yet
- The Flixborough, UK, Cyclohexane Disaster, 1 June 74Document24 pagesThe Flixborough, UK, Cyclohexane Disaster, 1 June 74rodofgodNo ratings yet
- Flixborough Disaster (1974) : A.K. GuptaDocument24 pagesFlixborough Disaster (1974) : A.K. GuptamkkamarajNo ratings yet
- Flixborough DisasterDocument4 pagesFlixborough DisasterEddylyn MarieNo ratings yet
- Learning From ECS Failures: What Can Go Wrong?: Fall 2012 Lecture # XXDocument19 pagesLearning From ECS Failures: What Can Go Wrong?: Fall 2012 Lecture # XXHeru HermansyahNo ratings yet
- Nuclear Reactor Meltdown: The Chernobyl DisasterDocument31 pagesNuclear Reactor Meltdown: The Chernobyl DisasterZim Vicom100% (1)
- ChernobylDocument34 pagesChernobylShivam Mishra100% (1)
- Flixborough Disaster PresentationDocument6 pagesFlixborough Disaster PresentationTan Yong ChaiNo ratings yet
- 4.3b Phillips SlidesDocument17 pages4.3b Phillips SlidesSrashti NemaNo ratings yet
- Chernobyl DisasterDocument13 pagesChernobyl DisasterDRISTIE KALITANo ratings yet
- A Seminar Presentation ON BY Deep Das ROLL NO - 202115009: "Flixborough Disaster"Document13 pagesA Seminar Presentation ON BY Deep Das ROLL NO - 202115009: "Flixborough Disaster"SabariMechyNo ratings yet
- Flixborough DisasterDocument20 pagesFlixborough DisasterEshan BhatNo ratings yet
- When Isolations Go Wrong: 5 Case Studies on Isolation FailuresDocument44 pagesWhen Isolations Go Wrong: 5 Case Studies on Isolation FailuresenriqueramoscNo ratings yet
- FlixboroughDocument9 pagesFlixboroughqemaismailNo ratings yet
- HHW CommerceDocument19 pagesHHW CommerceSickoNo ratings yet
- ChallengerDocument21 pagesChallengersharda121No ratings yet
- CHERNOBYL DISASTER: THE 1986 NUCLEAR ACCIDENTDocument15 pagesCHERNOBYL DISASTER: THE 1986 NUCLEAR ACCIDENT149Yashraj PrasadNo ratings yet
- Nuclear Energy: A Hell of a Way to Boil WaterDocument22 pagesNuclear Energy: A Hell of a Way to Boil WaterSesilia RockwoodNo ratings yet
- Flixborough (UK) 197402 0Document13 pagesFlixborough (UK) 197402 0Emma Slater100% (1)
- A Brief History of Nuclear Accidents Worldwide - Union of Concerned ScientistsDocument4 pagesA Brief History of Nuclear Accidents Worldwide - Union of Concerned ScientistsAjay SharmaNo ratings yet
- LPG General Product and Emergency Response TrainingDocument84 pagesLPG General Product and Emergency Response TrainingWasim AshfaqNo ratings yet
- Disaster Case StudyDocument13 pagesDisaster Case Study76 NISHANT RANANo ratings yet
- Texas City, TX: Amanda EnglerDocument27 pagesTexas City, TX: Amanda EnglerPrajay ShahNo ratings yet
- O2gg2u8segwzn02ook1z Signature Poli 150707151811 Lva1 App6891Document32 pagesO2gg2u8segwzn02ook1z Signature Poli 150707151811 Lva1 App6891machz0No ratings yet
- Chernobyl Disaster: Saurabh Bhavsar Ameya Borwankar Akshay Chaubal Rohan ChaukulkarDocument17 pagesChernobyl Disaster: Saurabh Bhavsar Ameya Borwankar Akshay Chaubal Rohan ChaukulkarRamu KrishnanNo ratings yet
- Chernobyltragedy 110120013647 Phpapp01Document17 pagesChernobyltragedy 110120013647 Phpapp01machz0No ratings yet
- Case StudyDocument18 pagesCase StudyRaja MohsinNo ratings yet
- Flixborough Incident of 1974Document15 pagesFlixborough Incident of 1974shaktipal singh DeoraNo ratings yet
- TEPCO's Nuclear Power Plantssuffered From Big Earthquake Ofmarch 11,2011Document22 pagesTEPCO's Nuclear Power Plantssuffered From Big Earthquake Ofmarch 11,2011EnformableNo ratings yet
- Major failure at Browns Ferry Nuclear Power Plant in 1975Document7 pagesMajor failure at Browns Ferry Nuclear Power Plant in 1975Saad AliNo ratings yet
- ChernobylDocument5 pagesChernobylAnonymous V0ttRnNo ratings yet
- Investigation Reportsuncor Altares PDFDocument12 pagesInvestigation Reportsuncor Altares PDFR GunalanNo ratings yet
- EVS Assignment Nuclear DisastersDocument4 pagesEVS Assignment Nuclear DisastersakhilvighNo ratings yet
- It All Started On Friday, 11 March 2011, 2.46 PMDocument8 pagesIt All Started On Friday, 11 March 2011, 2.46 PMYu ChengNo ratings yet
- Chernobyl DisasterDocument16 pagesChernobyl DisasterGeeNo ratings yet
- Chernobyl Disaster: 400x Fallout of HiroshimaDocument5 pagesChernobyl Disaster: 400x Fallout of Hiroshima6163 SHARANYA SNo ratings yet
- Case Studies For FinalDocument8 pagesCase Studies For FinalDule NilkNo ratings yet
- The Challenger Disaster A Case-Study in Engineering EthicsDocument18 pagesThe Challenger Disaster A Case-Study in Engineering EthicsAishwarya MurukesanNo ratings yet
- Assistant Professor Organic Chemistry Division, SAS, VIT University, Vellore - 14Document33 pagesAssistant Professor Organic Chemistry Division, SAS, VIT University, Vellore - 14RiajiminNo ratings yet
- ChernobylDocument4 pagesChernobylhweta173No ratings yet
- Flixborough Disaster 1974Document12 pagesFlixborough Disaster 1974Gladice ann mejiaNo ratings yet
- Introduction Soc 101Document21 pagesIntroduction Soc 101Shelly EfedhomaNo ratings yet
- Unit C Element 2Document10 pagesUnit C Element 2w hiteNo ratings yet
- Fukushima Event - FPLSummaryDocument14 pagesFukushima Event - FPLSummaryJulendra AriatedjaNo ratings yet
- UNIT IV Nuclear Power PlantDocument54 pagesUNIT IV Nuclear Power Plantsai venkatsharmaNo ratings yet
- 3) EX 5,02. Accident Analysis ExerciseDocument6 pages3) EX 5,02. Accident Analysis ExerciseAndrejSukoraNo ratings yet
- Flixborough - Event DiscussionDocument4 pagesFlixborough - Event DiscussionOnee chanNo ratings yet
- Challenger Disaster Case Study: O-Ring Failure & NASA PressureDocument11 pagesChallenger Disaster Case Study: O-Ring Failure & NASA PressureDeepa DhilipNo ratings yet
- The Accident in Bhopal: Observations 20 Years LaterDocument58 pagesThe Accident in Bhopal: Observations 20 Years LaterntpckanihaNo ratings yet
- Reformer Tube Failure IDocument13 pagesReformer Tube Failure Iabhijitwakodikar100% (2)
- Piper Alpha Background & ShortcomingsDocument4 pagesPiper Alpha Background & Shortcomingsfashwin0% (1)
- Challenger Case StudyDocument12 pagesChallenger Case StudySudeep JasonNo ratings yet
- Chernobyl Disaster: The Worst Manmade Disaster in Human HistoryDocument18 pagesChernobyl Disaster: The Worst Manmade Disaster in Human HistoryNeelam ChhipaNo ratings yet
- Chernobyl-Catastrophic Nuclear Incident:: What Was The Accident?Document2 pagesChernobyl-Catastrophic Nuclear Incident:: What Was The Accident?banitaNo ratings yet
- Nuclear Disasters: Three Mile IslandDocument5 pagesNuclear Disasters: Three Mile IslandSekhar VelampalliNo ratings yet
- Welcome: One Day Seminar OnDocument47 pagesWelcome: One Day Seminar Onshindesv2000No ratings yet
- Thin Safety Margin: The SEFOR Super-Prompt-Critical Transient Experiments, Ozark Mountains, Arkansas, 1970–71From EverandThin Safety Margin: The SEFOR Super-Prompt-Critical Transient Experiments, Ozark Mountains, Arkansas, 1970–71No ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Tugas Matematika Teknik PDFDocument2 pagesTugas Matematika Teknik PDFayukurnNo ratings yet
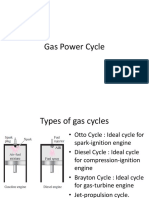
- Kuliah 11agas Power CycleDocument20 pagesKuliah 11agas Power CycleayukurnNo ratings yet
- Journal of Chromatography A Volume Issue 2017 (Doi 10.1016 - J.chroma.2017.05.035) Nestola, Marco Schmidt, Torsten C. - Determination of Mineral Oil Aromatic Hydrocarbons (MOAH) in Edible Oils and FDocument21 pagesJournal of Chromatography A Volume Issue 2017 (Doi 10.1016 - J.chroma.2017.05.035) Nestola, Marco Schmidt, Torsten C. - Determination of Mineral Oil Aromatic Hydrocarbons (MOAH) in Edible Oils and FayukurnNo ratings yet
- Tugas Matematika TeknikDocument2 pagesTugas Matematika TeknikayukurnNo ratings yet
- A Rapid and Sensitive Profiling of Free Fatty AcidDocument10 pagesA Rapid and Sensitive Profiling of Free Fatty AcidayukurnNo ratings yet
- Journal of Food and Drug Analysis Volume Issue 2018 (Doi 10.1016 - J.jfda.2018.06.008) Yazgan Karacaglar, Nazife Nur Bulat, Tugba Boyaci, Ismail Hakk - Raman Spectroscopy Coupled With Chemometric MDocument10 pagesJournal of Food and Drug Analysis Volume Issue 2018 (Doi 10.1016 - J.jfda.2018.06.008) Yazgan Karacaglar, Nazife Nur Bulat, Tugba Boyaci, Ismail Hakk - Raman Spectroscopy Coupled With Chemometric MayukurnNo ratings yet
- Food Control Volume Issue 2018 (Doi 10.1016 - J.foodcont.2018.03.046) Guyader, Sophie Thomas, Freddy Portaluri, Vincent Jamin, Eric - Authentication of Edible Fats and Oils by Non-Targeted 13 C inDocument24 pagesFood Control Volume Issue 2018 (Doi 10.1016 - J.foodcont.2018.03.046) Guyader, Sophie Thomas, Freddy Portaluri, Vincent Jamin, Eric - Authentication of Edible Fats and Oils by Non-Targeted 13 C inayukurnNo ratings yet
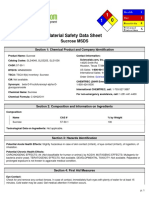
- Health and Safety Data for SucroseDocument5 pagesHealth and Safety Data for SucroseSilvi TatianNo ratings yet
- NHBC Standards 2011 Bre SD 1 SRCDocument5 pagesNHBC Standards 2011 Bre SD 1 SRCSuresh RaoNo ratings yet
- Nursing Grand Rounds Reviewer PDFDocument17 pagesNursing Grand Rounds Reviewer PDFAlyssa Jade GolezNo ratings yet
- California Evaluation Procedures For New Aftermarket Catalytic ConvertersDocument27 pagesCalifornia Evaluation Procedures For New Aftermarket Catalytic Convertersferio252No ratings yet
- How Nokia Failed to Adapt to Market ChangesDocument5 pagesHow Nokia Failed to Adapt to Market ChangesRiangelli ExcondeNo ratings yet
- Principles of Marketing Handout 4: Marketing Opportunity and Consumer AnalysisDocument19 pagesPrinciples of Marketing Handout 4: Marketing Opportunity and Consumer AnalysisAsset Dy100% (1)
- Tribology Aspects in Angular Transmission Systems: Hypoid GearsDocument7 pagesTribology Aspects in Angular Transmission Systems: Hypoid GearspiruumainNo ratings yet
- CCST+Cybersecurity+Objecitve+Domain Cisco Final wCiscoLogoDocument3 pagesCCST+Cybersecurity+Objecitve+Domain Cisco Final wCiscoLogoQazi ZayadNo ratings yet
- Seasonal Work Brochure 05Document2 pagesSeasonal Work Brochure 05R-lau R-pizNo ratings yet
- EY - NASSCOM - M&A Trends and Outlook - Technology Services VF - 0Document35 pagesEY - NASSCOM - M&A Trends and Outlook - Technology Services VF - 0Tejas JosephNo ratings yet
- Manual Equus 810 070Document10 pagesManual Equus 810 070Juan Ramón100% (1)
- Datasheet of DS 7608NI Q1 - 8P NVRD - V4.71.200 - 20220705Document5 pagesDatasheet of DS 7608NI Q1 - 8P NVRD - V4.71.200 - 20220705Gherel TocasNo ratings yet
- Floor MatsDocument3 pagesFloor MatsGhayas JawedNo ratings yet
- ChecklistDocument2 pagesChecklistKyra AlesonNo ratings yet
- Proximate Cause ExplainedDocument3 pagesProximate Cause ExplainedJoanne BayyaNo ratings yet
- Lentz Criminal ComplaintDocument16 pagesLentz Criminal ComplaintKristen Faith SchneiderNo ratings yet
- Total Standards: - Total Sub-Standards: - Total ESR StandardsDocument8 pagesTotal Standards: - Total Sub-Standards: - Total ESR StandardsHCX dghhqNo ratings yet
- Chapter 6Document53 pagesChapter 6Sam KhanNo ratings yet
- Certified Elder Law Attorney Middletown NyDocument8 pagesCertified Elder Law Attorney Middletown NymidhudsonlawNo ratings yet
- Personal Styling Service-Contract - No WatermarkDocument5 pagesPersonal Styling Service-Contract - No WatermarkLexine Emille100% (1)
- BS 3892-1 1997 - Pulverized-Fuel AshDocument22 pagesBS 3892-1 1997 - Pulverized-Fuel Ashmykel_dp100% (1)
- MSCL PipeDocument9 pagesMSCL PipeAhmad Zakwan Asmad100% (1)
- Younis 2020Document5 pagesYounis 2020nalakathshamil8No ratings yet
- Russian Federation Country Codes from World Development IndicatorsDocument262 pagesRussian Federation Country Codes from World Development IndicatorsMuhammad Talha TalhaNo ratings yet
- Analysis and Design of BeamsDocument12 pagesAnalysis and Design of BeamsHasanain AlmusawiNo ratings yet
- Manipulative MediaDocument15 pagesManipulative MediaCris Popol100% (2)
- Vodacom Fibre - Application Form CPD - 23 August 2018Document8 pagesVodacom Fibre - Application Form CPD - 23 August 2018Mla Emmanuel ZondoNo ratings yet
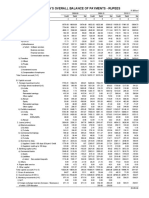
- Table 141: India'S Overall Balance of Payments - RupeesDocument2 pagesTable 141: India'S Overall Balance of Payments - Rupeesmahbobullah rahmaniNo ratings yet
- Informe de FallasDocument7 pagesInforme de FallasMiriam Maribel Torres SaguaNo ratings yet
- AI Writing Tools For Social Media Marketing Creating Compelling PostsDocument5 pagesAI Writing Tools For Social Media Marketing Creating Compelling PostsJames DanielsNo ratings yet
- Lecture 08Document27 pagesLecture 08simraNo ratings yet