You might also like
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersFrom EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersNo ratings yet
- 12 - Objective RefractionDocument11 pages12 - Objective RefractionSumon SarkarNo ratings yet
- Astigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAstigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Refraction and AccommodationDocument80 pagesRefraction and Accommodationapi-19916399100% (2)
- College of Medicine and Health Science, Department of OptometryDocument47 pagesCollege of Medicine and Health Science, Department of Optometryhenok birukNo ratings yet
- Binocular vision anomalies overviewDocument13 pagesBinocular vision anomalies overviewblueiceNo ratings yet
- 13 Programme Handbook MSC Clinical Optometry Feb 13Document94 pages13 Programme Handbook MSC Clinical Optometry Feb 13phenixousNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Orthoptic Exercises for OptometristsDocument6 pagesOrthoptic Exercises for OptometristsCatalin GeorgeNo ratings yet
- Congenital Strabismus: S. Vanitha, B.optom, 3 YearDocument23 pagesCongenital Strabismus: S. Vanitha, B.optom, 3 YearDivya Priya Dharmalingam100% (1)
- Binocular Vision Anomalies: Symptomatic HeterophoriaDocument10 pagesBinocular Vision Anomalies: Symptomatic HeterophoriaGraham CoffeyNo ratings yet
- Essential Perimetry The Field Analyzer PrimerDocument162 pagesEssential Perimetry The Field Analyzer PrimerDavid Croes100% (1)
- Far-Sightedness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFar-Sightedness, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamNo ratings yet
- Everything You Need to Know About Strabismus Diagnosis and TreatmentDocument197 pagesEverything You Need to Know About Strabismus Diagnosis and TreatmentRaluca OpreaNo ratings yet
- Diplopia (Double Vision), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiplopia (Double Vision), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- The Spotty RetinaDocument5 pagesThe Spotty RetinaJose Luis Mato AhcanNo ratings yet
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsFrom EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo ratings yet
- Case Studies PresbyopiaDocument33 pagesCase Studies PresbyopiaMalaika ZubairNo ratings yet
- Glaucoma and Ocular HypertensionDocument6 pagesGlaucoma and Ocular HypertensionsoniasistNo ratings yet
- ITP2Document42 pagesITP2Mehak JainNo ratings yet
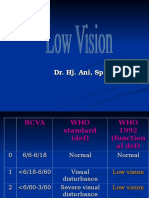
- Low VisionDocument36 pagesLow VisionIqbal HabibieNo ratings yet
- Cycloplegic Retinoscopy in InfancyDocument5 pagesCycloplegic Retinoscopy in InfancyStrauss de LangeNo ratings yet
- Paediatric Optometry Part 1 exam answersDocument5 pagesPaediatric Optometry Part 1 exam answersSourav KarmakarNo ratings yet
- Clinical Orthoptics - Fiona Rowe - 146Document6 pagesClinical Orthoptics - Fiona Rowe - 146Danielle SangalangNo ratings yet
- Keratometer Easy To Understand PDFDocument2 pagesKeratometer Easy To Understand PDFDanielle SangalangNo ratings yet
- Foreign Optometrist For CanadaDocument9 pagesForeign Optometrist For CanadaABDUL HAMEEDNo ratings yet
- FC Ophth (SA) Primary IA Past Papers - 2019 1st Semester 18-3-2019Document2 pagesFC Ophth (SA) Primary IA Past Papers - 2019 1st Semester 18-3-2019Richard100% (1)
- Right Hand Column Guide to Eye Exam EssentialsDocument3 pagesRight Hand Column Guide to Eye Exam Essentialssharu4291No ratings yet
- Third Years Log BookDocument11 pagesThird Years Log BookMeenakshi Kumar100% (2)
- 16.retinal Detachment PDFDocument42 pages16.retinal Detachment PDFFrederica MutiaraNo ratings yet
- Clinical Case in Contact Lenses, 1e - 2001Document205 pagesClinical Case in Contact Lenses, 1e - 2001Miguel PalaciosNo ratings yet
- Nungki-Esodeviations & ExodeviationsDocument36 pagesNungki-Esodeviations & ExodeviationsNia RoosdhantiaNo ratings yet
- Investigative Techniques & Ocular Examination - Sandip DoshiDocument161 pagesInvestigative Techniques & Ocular Examination - Sandip DoshiShifan Abdul MajeedNo ratings yet
- Viva and Osce Exams in Ophthalmology A Revision Study Guide 1st Ed 9783030430627 9783030430634 CompressDocument392 pagesViva and Osce Exams in Ophthalmology A Revision Study Guide 1st Ed 9783030430627 9783030430634 CompressstingbeesparvNo ratings yet
- Pediatric Eye Examination: Seia MahananiDocument35 pagesPediatric Eye Examination: Seia MahananiRaissaNo ratings yet
- Clinical OpticsDocument88 pagesClinical OpticsKris ArchibaldNo ratings yet
- 17.vitreous Opacities PDFDocument8 pages17.vitreous Opacities PDFPutri Dwi KartiniNo ratings yet
- Passed Arab Board Exam 2014 with Recommended ReferencesDocument5 pagesPassed Arab Board Exam 2014 with Recommended ReferencesMuhammed AbdulmajeedNo ratings yet
- 2735 Pediatric Cataract Manual - CompressedDocument66 pages2735 Pediatric Cataract Manual - CompressedKevin RamsahaiNo ratings yet
- CORNEA Vision2020 DR - RajarathnaDocument7 pagesCORNEA Vision2020 DR - Rajarathnaadi100% (1)
- Retinal Detachment SlideDocument54 pagesRetinal Detachment SlideHerin NataliaNo ratings yet
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamNo ratings yet
- Lens and CataractDocument55 pagesLens and CataractRold Brio Sos100% (1)
- Examination of The Eye: Xiaohui Zhao MD - Phd. Wuhan University Renmin HospitalDocument26 pagesExamination of The Eye: Xiaohui Zhao MD - Phd. Wuhan University Renmin Hospitalapi-19641337No ratings yet
- Basic Sciences in Ophthalmology - 9788184486087-EmailDocument446 pagesBasic Sciences in Ophthalmology - 9788184486087-EmailwulanfarichahNo ratings yet
- Lasers in Ophthalmology Part - 1Document53 pagesLasers in Ophthalmology Part - 1bhartiNo ratings yet
- New in OrthopticsDocument5 pagesNew in Orthopticsgargi.c100% (2)
- ICO-OSCAR Surgical AssessmentDocument4 pagesICO-OSCAR Surgical Assessmentzaidoonys1No ratings yet
- CLP Topic 5 Rigid Gas Permeable (RGP) Lens Fitting EvaluationDocument26 pagesCLP Topic 5 Rigid Gas Permeable (RGP) Lens Fitting EvaluationRhendy 172019022No ratings yet
- Atlas of Optic Nerve Head Evaluation in Glaucoma PDFDocument134 pagesAtlas of Optic Nerve Head Evaluation in Glaucoma PDFJosé MiguelNo ratings yet
- Module 5 - Ocular Motility - Cover TestDocument12 pagesModule 5 - Ocular Motility - Cover TestCat Loved KirariNo ratings yet
- Incomitant SquintDocument41 pagesIncomitant Squintshreeja maheshwari100% (3)
- Quartz 9000 Future 5w-30Document1 pageQuartz 9000 Future 5w-30awaisNo ratings yet
- Online Opticians UK Glasses Reglaze Order Form PDFDocument2 pagesOnline Opticians UK Glasses Reglaze Order Form PDFawaisNo ratings yet
- STD Subj Refract Plus Cyl CliniciansDocument8 pagesSTD Subj Refract Plus Cyl CliniciansawaisNo ratings yet
- Kolker SubjectiveRefraction PressReleaseDocument1 pageKolker SubjectiveRefraction PressReleaseawais100% (1)
- Correct Spherical Errors with Subjective RefractionDocument11 pagesCorrect Spherical Errors with Subjective RefractionMagfirah HalimNo ratings yet
- STD Subj Refract Plus MinusCyl ClinicansDocument12 pagesSTD Subj Refract Plus MinusCyl ClinicansawaisNo ratings yet
- Refraction and PrescribingDocument6 pagesRefraction and PrescribingawaisNo ratings yet
- STD Subj Refract MinusCyl CliniciansDocument8 pagesSTD Subj Refract MinusCyl CliniciansawaisNo ratings yet
- Cold Chain Distribution Issues at Indo-Euro PharmaDocument19 pagesCold Chain Distribution Issues at Indo-Euro Pharmaely100% (2)
- Movie Review - Seven Sundays (Barredo)Document2 pagesMovie Review - Seven Sundays (Barredo)Julienne BarredoNo ratings yet
- Cestodes TableDocument3 pagesCestodes TableSuha AbdullahNo ratings yet
- Chemical Fact SheetDocument2 pagesChemical Fact SheetAnonymous dp5b3X1NANo ratings yet
- Guymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaDocument93 pagesGuymer Giant Cell Arteritis Polymyalgia Rheumatica FibromyalgiaKe Xu100% (1)
- Journal of Traditional and Complementary Medicine: Marhasiyah Rahim, Foong Kiew Ooi, Wan Zuraida Wan Abdul HamidDocument7 pagesJournal of Traditional and Complementary Medicine: Marhasiyah Rahim, Foong Kiew Ooi, Wan Zuraida Wan Abdul HamidKholifatur RohmaNo ratings yet
- Ibuprofen Effect on Osteoblast ProliferationDocument7 pagesIbuprofen Effect on Osteoblast ProliferationGilliam SierraNo ratings yet
- ResearcfhSleep DeprivationDocument36 pagesResearcfhSleep DeprivationDonna CatantanNo ratings yet
- Step 1 Checklist for Biochemistry, Genetics and DevelopmentDocument11 pagesStep 1 Checklist for Biochemistry, Genetics and DevelopmentHasan Khan RoudbaryNo ratings yet
- C Difficile SporesDocument3 pagesC Difficile SporesEda SopNo ratings yet
- Epidermal Permeability Barrier Defects and Barrier Repair Therapy in Atopic DermatitisDocument12 pagesEpidermal Permeability Barrier Defects and Barrier Repair Therapy in Atopic DermatitisMisaeldpdNo ratings yet
- MLS & IMT Reading List 3-13Document2 pagesMLS & IMT Reading List 3-13Joseph SabidoNo ratings yet
- Acquired and Developmental Disturbance of The Teeth andDocument80 pagesAcquired and Developmental Disturbance of The Teeth andyufita fitrianiNo ratings yet
- Chemical Carcinogenesis: Metabolic Activation, DNA Adducts, Multistage ModelDocument85 pagesChemical Carcinogenesis: Metabolic Activation, DNA Adducts, Multistage ModelNidyaletchmy ReddyNo ratings yet
- Print Kil DavidDocument9 pagesPrint Kil Davidapi-3806285No ratings yet
- Book Excerpt: 'Psychology's Ghost: The Crisis in The Profession and The Way Back'Document5 pagesBook Excerpt: 'Psychology's Ghost: The Crisis in The Profession and The Way Back'WBURNo ratings yet
- JR Science Quiz 19-20 Class VI - VIIIDocument43 pagesJR Science Quiz 19-20 Class VI - VIIIDAVV IQACNo ratings yet
- AS 1680.0-1998 Interior Lighting-Safe MovementDocument17 pagesAS 1680.0-1998 Interior Lighting-Safe Movementvxzvzxvzv0% (1)
- Plum ProductionDocument3 pagesPlum ProductionSharad BhutoriaNo ratings yet
- Conscious Sedation Guidelines for DentistsDocument18 pagesConscious Sedation Guidelines for DentistsAnna NgNo ratings yet
- TonsilitisDocument23 pagesTonsilitisCrisantaMadrid0% (1)
- Basics of Biostatistics PDFDocument31 pagesBasics of Biostatistics PDFDrAnisha PatelNo ratings yet
- Molar PregnancyDocument7 pagesMolar PregnancyFelix Valerian HalimNo ratings yet
- Human Skeleton NotesDocument29 pagesHuman Skeleton NotesSoumyajit DasNo ratings yet
- Acta Scientiae Veterinariae 1678-0345: Issn: Actascivet@Document5 pagesActa Scientiae Veterinariae 1678-0345: Issn: Actascivet@AlejandraNo ratings yet
- 2257 Model Release ForDocument2 pages2257 Model Release ForNitasha Tiku94% (17)
- EPEC PathogenDocument6 pagesEPEC Pathogenuypaul97No ratings yet
- TLE-HE (Dressmaking) : Activity Sheet Quarter 0 - MELC 4Document15 pagesTLE-HE (Dressmaking) : Activity Sheet Quarter 0 - MELC 4Mari PagxNo ratings yet
- Gram Positive Cocci Bacteriology ChartDocument2 pagesGram Positive Cocci Bacteriology ChartIsabella CeaNo ratings yet
- Patient Counselling - CPDocument8 pagesPatient Counselling - CPmrcopy xeroxNo ratings yet
- Build a Mathematical Mind - Even If You Think You Can't Have One: Become a Pattern Detective. Boost Your Critical and Logical Thinking Skills.From EverandBuild a Mathematical Mind - Even If You Think You Can't Have One: Become a Pattern Detective. Boost Your Critical and Logical Thinking Skills.Rating: 5 out of 5 stars5/5 (1)
- A Mathematician's Lament: How School Cheats Us Out of Our Most Fascinating and Imaginative Art FormFrom EverandA Mathematician's Lament: How School Cheats Us Out of Our Most Fascinating and Imaginative Art FormRating: 5 out of 5 stars5/5 (5)
- Quantum Physics: A Beginners Guide to How Quantum Physics Affects Everything around UsFrom EverandQuantum Physics: A Beginners Guide to How Quantum Physics Affects Everything around UsRating: 4.5 out of 5 stars4.5/5 (3)
- Mental Math Secrets - How To Be a Human CalculatorFrom EverandMental Math Secrets - How To Be a Human CalculatorRating: 5 out of 5 stars5/5 (3)
- Basic Math & Pre-Algebra Workbook For Dummies with Online PracticeFrom EverandBasic Math & Pre-Algebra Workbook For Dummies with Online PracticeRating: 4 out of 5 stars4/5 (2)
- Mathematical Mindsets: Unleashing Students' Potential through Creative Math, Inspiring Messages and Innovative TeachingFrom EverandMathematical Mindsets: Unleashing Students' Potential through Creative Math, Inspiring Messages and Innovative TeachingRating: 4.5 out of 5 stars4.5/5 (21)
- Making and Tinkering With STEM: Solving Design Challenges With Young ChildrenFrom EverandMaking and Tinkering With STEM: Solving Design Challenges With Young ChildrenNo ratings yet
- Limitless Mind: Learn, Lead, and Live Without BarriersFrom EverandLimitless Mind: Learn, Lead, and Live Without BarriersRating: 4 out of 5 stars4/5 (6)
- Fluent in 3 Months: How Anyone at Any Age Can Learn to Speak Any Language from Anywhere in the WorldFrom EverandFluent in 3 Months: How Anyone at Any Age Can Learn to Speak Any Language from Anywhere in the WorldRating: 3 out of 5 stars3/5 (79)
- A Mathematician's Lament: How School Cheats Us Out of Our Most Fascinating and Imaginative Art FormFrom EverandA Mathematician's Lament: How School Cheats Us Out of Our Most Fascinating and Imaginative Art FormRating: 4.5 out of 5 stars4.5/5 (20)
- A-level Maths Revision: Cheeky Revision ShortcutsFrom EverandA-level Maths Revision: Cheeky Revision ShortcutsRating: 3.5 out of 5 stars3.5/5 (8)
- Strategies for Problem Solving: Equip Kids to Solve Math Problems With ConfidenceFrom EverandStrategies for Problem Solving: Equip Kids to Solve Math Problems With ConfidenceNo ratings yet
- Calculus Workbook For Dummies with Online PracticeFrom EverandCalculus Workbook For Dummies with Online PracticeRating: 3.5 out of 5 stars3.5/5 (8)
- Classroom-Ready Number Talks for Kindergarten, First and Second Grade Teachers: 1,000 Interactive Activities and Strategies that Teach Number Sense and Math FactsFrom EverandClassroom-Ready Number Talks for Kindergarten, First and Second Grade Teachers: 1,000 Interactive Activities and Strategies that Teach Number Sense and Math FactsNo ratings yet