You might also like
- Objective Refraction Technique: Retinoscopy: Aao ReadingDocument57 pagesObjective Refraction Technique: Retinoscopy: Aao ReadingKhairunnisaNo ratings yet
- Retinoscope & RetinosDocument41 pagesRetinoscope & RetinosMiriam Mwangi100% (1)
- Astigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAstigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Optigal's Q & A for the NOCE: National Opticianry Certification Exam Questions - Basic CertificationFrom EverandOptigal's Q & A for the NOCE: National Opticianry Certification Exam Questions - Basic CertificationNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Visual Optics 1,2.......Document468 pagesVisual Optics 1,2.......henok birukNo ratings yet
- Orthoptic Exercises for OptometristsDocument6 pagesOrthoptic Exercises for OptometristsCatalin GeorgeNo ratings yet
- CLP Topic 5 Rigid Gas Permeable (RGP) Lens Fitting EvaluationDocument26 pagesCLP Topic 5 Rigid Gas Permeable (RGP) Lens Fitting EvaluationRhendy 172019022No ratings yet
- Bifocal Contact Lenses PDFDocument10 pagesBifocal Contact Lenses PDFLauw Dwi AndrikNo ratings yet
- RefraksiDocument84 pagesRefraksinaroetocapkutilNo ratings yet
- LASIK EmergenciesDocument187 pagesLASIK EmergenciesMike LadhaNo ratings yet
- Binocular vision anomalies overviewDocument13 pagesBinocular vision anomalies overviewblueiceNo ratings yet
- Clinical Pocket Guide 2014 PDFDocument24 pagesClinical Pocket Guide 2014 PDFamitleckNo ratings yet
- Foreign Optometrist For CanadaDocument9 pagesForeign Optometrist For CanadaABDUL HAMEEDNo ratings yet
- CPG 19Document78 pagesCPG 19anon-24970100% (1)
- Night MiopiaDocument8 pagesNight MiopiamurilobsouzaNo ratings yet
- Everything You Need to Know About Strabismus Diagnosis and TreatmentDocument197 pagesEverything You Need to Know About Strabismus Diagnosis and TreatmentRaluca OpreaNo ratings yet
- Binocular Vision Anomalies: Symptomatic HeterophoriaDocument10 pagesBinocular Vision Anomalies: Symptomatic HeterophoriaGraham CoffeyNo ratings yet
- Clinical Optics ReviewDocument69 pagesClinical Optics ReviewnanpatelNo ratings yet
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsFrom EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsNo ratings yet
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersFrom EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersNo ratings yet
- Contact Lenses Chemicals, Methods, and Applications PDFDocument448 pagesContact Lenses Chemicals, Methods, and Applications PDFantonioNo ratings yet
- The Skeffington Perspective of the Behavioral Model of Optometric Data Analysis and Vision CareFrom EverandThe Skeffington Perspective of the Behavioral Model of Optometric Data Analysis and Vision CareNo ratings yet
- The Slit Lamp ExamDocument30 pagesThe Slit Lamp Examrapid73No ratings yet
- Contact Lenses For ChildrenDocument6 pagesContact Lenses For ChildrenmelikebooksNo ratings yet
- Clinical OpticsDocument88 pagesClinical OpticsKris ArchibaldNo ratings yet
- AniseikoniaDocument40 pagesAniseikoniahenok biruk100% (1)
- Myopia ManualDocument337 pagesMyopia ManualRealPurgatory100% (1)
- The Spotty RetinaDocument5 pagesThe Spotty RetinaJose Luis Mato AhcanNo ratings yet
- Paediatric Optometry Part 1 exam answersDocument5 pagesPaediatric Optometry Part 1 exam answersSourav KarmakarNo ratings yet
- PPP Refractive Error & Refractive Surgery PDFDocument104 pagesPPP Refractive Error & Refractive Surgery PDFMia NursalamahNo ratings yet
- Nungki-Esodeviations & ExodeviationsDocument36 pagesNungki-Esodeviations & ExodeviationsNia RoosdhantiaNo ratings yet
- Refraction and AccommodationDocument80 pagesRefraction and Accommodationapi-19916399100% (2)
- KeratometryDocument3 pagesKeratometrycarol_marie_3No ratings yet
- ITP2Document42 pagesITP2Mehak JainNo ratings yet
- Understanding Aberrometry for Eye CareDocument54 pagesUnderstanding Aberrometry for Eye Caresightbd100% (2)
- Measuring Lenses with a Lensometer & Lens Clock/GaugeDocument53 pagesMeasuring Lenses with a Lensometer & Lens Clock/GaugeManmohan Shah100% (1)
- Cycloplegic Retinoscopy in InfancyDocument5 pagesCycloplegic Retinoscopy in InfancyStrauss de LangeNo ratings yet
- Refractive Surgery PPP PDFDocument75 pagesRefractive Surgery PPP PDFdheerajkumarsahNo ratings yet
- Retinal Detachment SlideDocument54 pagesRetinal Detachment SlideHerin NataliaNo ratings yet
- Optometry PresentationDocument11 pagesOptometry PresentationEvelyn Tran100% (1)
- Cycloplegic Refraction in Optometric Practice 1337594763401 2Document14 pagesCycloplegic Refraction in Optometric Practice 1337594763401 2Strauss de LangeNo ratings yet
- Contact Lens Design Tables: Tables for the Determination of Surface Radii of Curvature of Hard Contact Lenses to Give a Required Axial Edge LiftFrom EverandContact Lens Design Tables: Tables for the Determination of Surface Radii of Curvature of Hard Contact Lenses to Give a Required Axial Edge LiftNo ratings yet
- Bennett and Rabbetts Clinical Visual OpticsDocument472 pagesBennett and Rabbetts Clinical Visual OpticsShifan Abdul MajeedNo ratings yet
- NATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideFrom EverandNATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideNo ratings yet
- Optics and Refraction For PodcastDocument75 pagesOptics and Refraction For Podcastapi-213285088No ratings yet
- KERATOCONUSDocument22 pagesKERATOCONUSAarush DeoraNo ratings yet
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamNo ratings yet
- Refractive Surgery (HJ) UpdatedDocument47 pagesRefractive Surgery (HJ) UpdatedSayoki ghosg100% (1)
- Clinical Orthoptics - Fiona Rowe - 146Document6 pagesClinical Orthoptics - Fiona Rowe - 146Danielle SangalangNo ratings yet
- Contact Applanation TonometryDocument6 pagesContact Applanation TonometryAmirhosseinSamadzadehNo ratings yet
- Trial Sets and Trial FramesDocument16 pagesTrial Sets and Trial FramesJúnior AlvesNo ratings yet
- Case Studies PresbyopiaDocument33 pagesCase Studies PresbyopiaMalaika ZubairNo ratings yet
- Strabismus Quick GuideDocument4 pagesStrabismus Quick Guideghitza80100% (1)
- Grading Scales in OptometryDocument4 pagesGrading Scales in Optometrynaravichandran3662No ratings yet
- Anomalous Retinal Correspondence - Diagnostic Tests and TherapyDocument5 pagesAnomalous Retinal Correspondence - Diagnostic Tests and TherapySumon SarkarNo ratings yet
- Silo - Tips - How To Take An Ophthalmic HistoryDocument5 pagesSilo - Tips - How To Take An Ophthalmic HistorySumon SarkarNo ratings yet
- BD Community CU (Responses) - Form Responses 1Document1 pageBD Community CU (Responses) - Form Responses 1Sumon SarkarNo ratings yet
- Patient Health HistoryDocument2 pagesPatient Health HistorySumon SarkarNo ratings yet
- 2022-08-27 18 - 53 - 11.578Document1 page2022-08-27 18 - 53 - 11.578Sumon SarkarNo ratings yet
- O&A LetterDocument2 pagesO&A LetterSumon SarkarNo ratings yet
- 293 FullDocument9 pages293 FullSumon SarkarNo ratings yet
- RGP Lens MeasurementDocument5 pagesRGP Lens MeasurementSumon SarkarNo ratings yet
- Answer Key MST 1 OMT 354 CL2Document1 pageAnswer Key MST 1 OMT 354 CL2Sumon SarkarNo ratings yet
- CCLRU contact lens staining scaleDocument2 pagesCCLRU contact lens staining scaleSumon SarkarNo ratings yet
- Pediatric Contact Lenses GuideDocument6 pagesPediatric Contact Lenses GuideSumon SarkarNo ratings yet
- Epidemiological Overview of Preventable Blindness in India-A Focus On Vitamin A Deficiency Among Pre-School Children in IndianDocument20 pagesEpidemiological Overview of Preventable Blindness in India-A Focus On Vitamin A Deficiency Among Pre-School Children in IndianSumon SarkarNo ratings yet
- Anomalous Retinal Correspondence and Its SignificanceDocument17 pagesAnomalous Retinal Correspondence and Its SignificanceSumon SarkarNo ratings yet
- Epidemiology With Part 2 (Complete) 2Document59 pagesEpidemiology With Part 2 (Complete) 2nahNo ratings yet
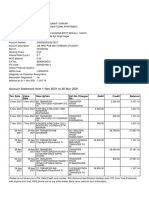
- Account Statement From 1 Nov 2021 To 30 Nov 2021: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceDocument2 pagesAccount Statement From 1 Nov 2021 To 30 Nov 2021: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceSumon SarkarNo ratings yet
- The Importance of Epidemiology in Optometry: Oriahi, M. ODocument4 pagesThe Importance of Epidemiology in Optometry: Oriahi, M. OSumon SarkarNo ratings yet
- SynaptophoreDocument1 pageSynaptophoreSumon SarkarNo ratings yet
- Vision Screening - Dr. WagnerDocument37 pagesVision Screening - Dr. WagnerDien Doan QuangNo ratings yet
- Phase 1 Assignment 4Document4 pagesPhase 1 Assignment 4Sumon SarkarNo ratings yet
- Umc Meetings 6-6-2022 To 7-6-2022Document4 pagesUmc Meetings 6-6-2022 To 7-6-2022Sumon SarkarNo ratings yet
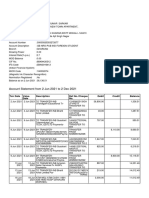
- Account Statement From 2 Jun 2021 To 2 Dec 2021: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceDocument9 pagesAccount Statement From 2 Jun 2021 To 2 Dec 2021: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceSumon SarkarNo ratings yet
- 21UCH-105 21UCH-105: Sr. NoDocument9 pages21UCH-105 21UCH-105: Sr. NoSumon SarkarNo ratings yet
- National Programme For Control of Blindness: Assistant Prof., Deptt. of Community Medicine GMCH ChandigarhDocument23 pagesNational Programme For Control of Blindness: Assistant Prof., Deptt. of Community Medicine GMCH ChandigarhSumon SarkarNo ratings yet
- National Programme For Control of Blindness & Visual ImpairmentDocument15 pagesNational Programme For Control of Blindness & Visual ImpairmentSumon SarkarNo ratings yet
- Uribapplicationform 67828132Document1 pageUribapplicationform 67828132Jignesh IoharNo ratings yet
- EPI-546 Block I Case-Control Studies LectureDocument32 pagesEPI-546 Block I Case-Control Studies LectureSumon SarkarNo ratings yet
- Assignment 3: Units 2.1, 2.2 and 2.3 of Module 2 of The IACLE Contact Lens CourseDocument5 pagesAssignment 3: Units 2.1, 2.2 and 2.3 of Module 2 of The IACLE Contact Lens CourseSumon SarkarNo ratings yet
- Uribapplicationform 67828132Document1 pageUribapplicationform 67828132Jignesh IoharNo ratings yet
- Semester 4Document15 pagesSemester 4Sumon SarkarNo ratings yet
- Aes 03 33Document7 pagesAes 03 33Sumon SarkarNo ratings yet
- Scaffold Inspection Checklist FINALDocument2 pagesScaffold Inspection Checklist FINALRhannie GarciaNo ratings yet
- Monetizing Judgments DatasheetDocument9 pagesMonetizing Judgments DatasheetJohnWilliams100% (4)
- Common Customer Gateway Product SheetDocument2 pagesCommon Customer Gateway Product SheetNYSE TechnologiesNo ratings yet
- Gerunds and Infinitives 8897Document3 pagesGerunds and Infinitives 8897aura lucy estupiñan gutierrezNo ratings yet
- Amarok 2011Document79 pagesAmarok 2011NPNo ratings yet
- Osamu Dazai: Genius, But No Saint - The Japan TimesDocument3 pagesOsamu Dazai: Genius, But No Saint - The Japan TimesBenito TenebrosusNo ratings yet
- Organic Agriculture Gr11 Q2.Module5 LRDocument17 pagesOrganic Agriculture Gr11 Q2.Module5 LRJam Hamil AblaoNo ratings yet
- An Introduction To The Study of Medieval Latin VersificationDocument246 pagesAn Introduction To The Study of Medieval Latin VersificationGregorio Gonzalez Moreda100% (1)
- Hoopvol Chapter Summaries PDFDocument29 pagesHoopvol Chapter Summaries PDFNakeisha Jesse Napallatan82% (28)
- A Street Car Named Desire (Penguin)Document18 pagesA Street Car Named Desire (Penguin)the_perfectionistNo ratings yet
- Geoboards in The ClassroomDocument37 pagesGeoboards in The ClassroomDanielle VezinaNo ratings yet
- İngilizce A1 Seviye FiillerDocument70 pagesİngilizce A1 Seviye FiillerMehmet DursunNo ratings yet
- Credits Is Hereby Given To Mrs. Jaylynne Escalona, Mscrim For Her Substantial Contribution As Regards To This NotesDocument15 pagesCredits Is Hereby Given To Mrs. Jaylynne Escalona, Mscrim For Her Substantial Contribution As Regards To This NoteseuniceNo ratings yet
- Activity Completion IN School-Based Seminar ON National Drug Education ProgramDocument12 pagesActivity Completion IN School-Based Seminar ON National Drug Education ProgramFATIMA APILADONo ratings yet
- Activity 3: Case Study Johnson & Johnson'S Stakeholder ApproachDocument3 pagesActivity 3: Case Study Johnson & Johnson'S Stakeholder ApproachNika CruzNo ratings yet
- Finals (3. LP) Termination and RepairDocument4 pagesFinals (3. LP) Termination and RepairAmelyn Goco MañosoNo ratings yet
- ch-1 Phy MEASUREMENT AND MOTIONDocument2 pagesch-1 Phy MEASUREMENT AND MOTIONRakesh GuptaNo ratings yet
- Korean Lesson PlanDocument4 pagesKorean Lesson Planapi-272316247No ratings yet
- Chapter 3Document76 pagesChapter 3Cha Boon KitNo ratings yet
- IAII FINAL EXAM Maual SET BDocument9 pagesIAII FINAL EXAM Maual SET BClara MacallingNo ratings yet
- Review Jurnal Halo EffectDocument12 pagesReview Jurnal Halo Effectadinda veradinaNo ratings yet
- Anuraj JainDocument3 pagesAnuraj Jainanuraj1983No ratings yet
- Jbe - Consent Readiness RelationshipsDocument4 pagesJbe - Consent Readiness Relationshipsapi-537847223No ratings yet
- 15-5240 enDocument14 pages15-5240 enRafa Lopez PuigdollersNo ratings yet
- Shadow On The Mountain Reading GuideDocument2 pagesShadow On The Mountain Reading GuideAbrams BooksNo ratings yet
- Subtraction Strategies That Lead To RegroupingDocument6 pagesSubtraction Strategies That Lead To Regroupingapi-171857844100% (1)
- PRACTICE-10 BảnDocument5 pagesPRACTICE-10 BảnBinh Pham ThanhNo ratings yet
- Hill Et Al 2013 Evol Hum BehavDocument8 pagesHill Et Al 2013 Evol Hum BehavMike WillieNo ratings yet
- Humanistic & Behavioural Approches To Counseling: Lekshmi Priya.K.B 2 MSC Applied PsychologyDocument49 pagesHumanistic & Behavioural Approches To Counseling: Lekshmi Priya.K.B 2 MSC Applied PsychologyAnand ChoubeyNo ratings yet
- ISE215 Lecture4 Usingtheproduct Andre SjsuDocument25 pagesISE215 Lecture4 Usingtheproduct Andre SjsuHALASA TextilHogarNo ratings yet