You might also like
- Halodoc Webinar On COVID 2020-03-21 V 0.4Document75 pagesHalodoc Webinar On COVID 2020-03-21 V 0.4Gabriella NelwanNo ratings yet
- COVID-19 Infection Prevention BasicsDocument46 pagesCOVID-19 Infection Prevention BasicsCainta Mpl Jail TanNo ratings yet
- CD NotesDocument7 pagesCD Notesstuffednurse100% (1)
- SlidesDocument150 pagesSlidesjiaraNo ratings yet
- Communicable Disease Nursing EssentialsDocument9 pagesCommunicable Disease Nursing EssentialsVied FranzuelaNo ratings yet
- Disaster NursingDocument30 pagesDisaster NursingRoman MamunNo ratings yet
- NOTES CD Lecture Generic 2022Document182 pagesNOTES CD Lecture Generic 2022Meryville JacildoNo ratings yet
- Seven Steps in Outbreak Investigation Including The Use of Relevant Epidemiological Methods - Health KnowledgeDocument7 pagesSeven Steps in Outbreak Investigation Including The Use of Relevant Epidemiological Methods - Health KnowledgeDinie BidiNo ratings yet
- Coronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowFrom EverandCoronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowNo ratings yet
- Pediatrics PresentationDocument18 pagesPediatrics Presentationapi-339903207No ratings yet
- Corona Virus: Information You Need and How to Protect Yourself and Your Fellow Human BeingsFrom EverandCorona Virus: Information You Need and How to Protect Yourself and Your Fellow Human BeingsNo ratings yet
- Communicable Disease NursingDocument7 pagesCommunicable Disease NursingNimrodNo ratings yet
- Tuberculosis Research Paper ExampleDocument4 pagesTuberculosis Research Paper Exampled1fytyt1man3100% (1)
- Causative Agents: Leon) (Flaviviruses) (Common in The Phil.) P. OvaleDocument12 pagesCausative Agents: Leon) (Flaviviruses) (Common in The Phil.) P. OvaleJUANJOSEFOXNo ratings yet
- Pandemic Influenza Toppenish School District Informational PresentationDocument31 pagesPandemic Influenza Toppenish School District Informational PresentationalnaturamilkaNo ratings yet
- Concepts of Infection ControlDocument61 pagesConcepts of Infection Controltummalapalli venkateswara rao100% (1)
- Clostridium Difficile Infection (CDI) : Prevention PrimerDocument80 pagesClostridium Difficile Infection (CDI) : Prevention PrimererpNo ratings yet
- Control of Viral Diseases: Derek WongDocument43 pagesControl of Viral Diseases: Derek WongAyioKunNo ratings yet
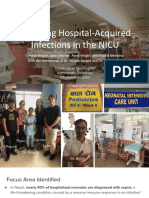
- Management of Outbreak in NICU - Lily RundjanDocument43 pagesManagement of Outbreak in NICU - Lily RundjanBayu KurniawanNo ratings yet
- ICPA Webinar Responding To Covid 19 in PrisonsDocument36 pagesICPA Webinar Responding To Covid 19 in PrisonsPriya RanjanNo ratings yet
- Avian and Pandemic Influenza: Infection Control PerspectivesDocument60 pagesAvian and Pandemic Influenza: Infection Control PerspectivesLavendra KunwarNo ratings yet
- DOH Emerging and Re Emerging Infectious DiseasesDocument51 pagesDOH Emerging and Re Emerging Infectious Diseasesnabsa100% (2)
- Infection Control Measures Epidemiology & Clinical ManagemeDocument29 pagesInfection Control Measures Epidemiology & Clinical ManagemeAnthony MoroNo ratings yet
- 4812 Volume 10 Transmission Based Precautions Isolation Guidelines PDFDocument29 pages4812 Volume 10 Transmission Based Precautions Isolation Guidelines PDFvabimhahNo ratings yet
- Diagnostic Tests: Leon) (Flaviviruses) (Common in The Phil.) P. OvaleDocument12 pagesDiagnostic Tests: Leon) (Flaviviruses) (Common in The Phil.) P. OvaleJUANJOSEFOXNo ratings yet
- HIV & AIDS PreventionDocument48 pagesHIV & AIDS PreventionkiookabNo ratings yet
- First Lecture - Infection Control - WrittenDocument25 pagesFirst Lecture - Infection Control - Writtenmohamed elshialNo ratings yet
- Communicable Disease Nursing Study BulletsDocument12 pagesCommunicable Disease Nursing Study Bulletsoh_chamieNo ratings yet
- Causative Agents: Leon) (Flaviviruses) (Common in The Phil.) P. OvaleDocument12 pagesCausative Agents: Leon) (Flaviviruses) (Common in The Phil.) P. OvaleJUANJOSEFOXNo ratings yet
- Drug Resistant TB - What Every Student Should Know: Elma de VriesDocument30 pagesDrug Resistant TB - What Every Student Should Know: Elma de VriesPhaimNo ratings yet
- TB Risk Prevention Emergency AreaDocument7 pagesTB Risk Prevention Emergency AreaalejandroNo ratings yet
- Contagion (Movie Review)Document5 pagesContagion (Movie Review)Stephy SalvadorNo ratings yet
- Public Health Science Nursing Practice 1st Edition Savage Test BankDocument12 pagesPublic Health Science Nursing Practice 1st Edition Savage Test Bankxuyenkeva3fon8100% (21)
- Public Health Science Nursing Practice 1St Edition Savage Test Bank Full Chapter PDFDocument33 pagesPublic Health Science Nursing Practice 1St Edition Savage Test Bank Full Chapter PDFanselmlayla3l3c1100% (6)
- Ohes4412 - 11Document27 pagesOhes4412 - 11AbdullahNo ratings yet
- Hospital Acquired InfectionsDocument51 pagesHospital Acquired Infectionstummalapalli venkateswara raoNo ratings yet
- Facts About h1n1 InfluenzaDocument20 pagesFacts About h1n1 InfluenzaSureshkumar ManoharanNo ratings yet
- Pandemic futures_3Document14 pagesPandemic futures_3bel.ikhtiarNo ratings yet
- Introduction to Public Health - Communicable Diseases, Prevention & ControlDocument57 pagesIntroduction to Public Health - Communicable Diseases, Prevention & ControlPeter CalvinsanNo ratings yet
- Transmission-Based PrecautionsDocument44 pagesTransmission-Based PrecautionsCharles FerdinandNo ratings yet
- 2013 NTP Manual Procedures for TB PreventionDocument32 pages2013 NTP Manual Procedures for TB PreventionaringkinkingNo ratings yet
- Cme On TuberclosisDocument12 pagesCme On TuberclosisOdulusi DanielNo ratings yet
- DD Cheat Sheet 21-22Document2 pagesDD Cheat Sheet 21-22loki anshNo ratings yet
- Sas Hes032 8Document8 pagesSas Hes032 8Jose Melmar Autida AutenticoNo ratings yet
- Prevention of Infection: Infectious Diseases Global HealthDocument12 pagesPrevention of Infection: Infectious Diseases Global HealthsaravananNo ratings yet
- In Respiratory Diseases: Triwahju Astuti Lab IP Paru & Respirasi FKUB-RSSA MalangDocument46 pagesIn Respiratory Diseases: Triwahju Astuti Lab IP Paru & Respirasi FKUB-RSSA MalangWan Adi OeyaNo ratings yet
- Chapter 12Document35 pagesChapter 12BRENDHIL PACIFICO CRUZNo ratings yet
- Part B 3 Influenza PandemicDocument5 pagesPart B 3 Influenza Pandemicfernanda1rondelliNo ratings yet
- 5.infection Control & Standard PrecautionsDocument33 pages5.infection Control & Standard PrecautionsGilbert JohnNo ratings yet
- Communicable Disease Prevention GuideDocument38 pagesCommunicable Disease Prevention GuideMazinNo ratings yet
- Intro To Epidemiology - SunpetchDocument95 pagesIntro To Epidemiology - SunpetchPASCALNo ratings yet
- 29 Nursing Management of Communicable DiseaseDocument79 pages29 Nursing Management of Communicable DiseaseMonika SanaaNo ratings yet
- Tuberculosis Thesis IntroductionDocument8 pagesTuberculosis Thesis Introductionifywpqvcf100% (2)
- Flu vs Stomach Bug: Key DifferencesDocument50 pagesFlu vs Stomach Bug: Key Differencesyash shrivastavaNo ratings yet
- Infection Control, Safety First Aid and Personal WellnessDocument9 pagesInfection Control, Safety First Aid and Personal WellnessJacinta MalamionNo ratings yet
- Communicating Science and Managing the Coronavirus PandemicFrom EverandCommunicating Science and Managing the Coronavirus PandemicNo ratings yet
- Introduction To EpiderminologyDocument27 pagesIntroduction To Epiderminologyoncolo10% (1)
- K.Hema Anandhy, M.SC Nursing, PuducherryDocument53 pagesK.Hema Anandhy, M.SC Nursing, PuducherryhemihemaNo ratings yet
- TuberculosisDocument20 pagesTuberculosisBader AljarboaNo ratings yet
- Qi Project-1Document10 pagesQi Project-1api-245887979No ratings yet
- WelcomeDocument5 pagesWelcomeCatNo ratings yet
- Assessment - First Step in The Nursing ProcessDocument4 pagesAssessment - First Step in The Nursing ProcessCynfully SweetNo ratings yet
- Asepsis and Infection ControlDocument15 pagesAsepsis and Infection ControlhannahNo ratings yet
- Community Nurses' Roles in Public HealthDocument3 pagesCommunity Nurses' Roles in Public HealthCynfully Sweet100% (1)
- CHN TextbookDocument313 pagesCHN TextbookCynfully SweetNo ratings yet
- Community Health Nursing: Additional NotesDocument5 pagesCommunity Health Nursing: Additional NotesCynfully SweetNo ratings yet
- 3 1bk04214aaaaDocument44 pages3 1bk04214aaaaAgus Hazelnut DiangeloNo ratings yet
- Comm HLTH NSG FinalDocument228 pagesComm HLTH NSG Finaljuly3ciaNo ratings yet
- Community Health Nursing: Additional NotesDocument5 pagesCommunity Health Nursing: Additional NotesCynfully SweetNo ratings yet
- Compliance CertificateDocument4 pagesCompliance CertificateCynfully SweetNo ratings yet
- CalendarDocument1 pageCalendarCynfully SweetNo ratings yet
- Instructions To Claimants - Pentagon and ShanksvilleDocument17 pagesInstructions To Claimants - Pentagon and ShanksvilleCynfully SweetNo ratings yet
- Infection Prevention and Emergency Management: Terri Rebmann, PHD, RN, Cic Associate ProfessorDocument51 pagesInfection Prevention and Emergency Management: Terri Rebmann, PHD, RN, Cic Associate ProfessorCynfully SweetNo ratings yet
- Infection Prevention and Emergency Management: Terri Rebmann, PHD, RN, Cic Associate ProfessorDocument51 pagesInfection Prevention and Emergency Management: Terri Rebmann, PHD, RN, Cic Associate ProfessorCynfully SweetNo ratings yet
- Monthly Health CalendarDocument4 pagesMonthly Health CalendarMercicae ANo ratings yet
- LPN Communicable DiseasesDocument4 pagesLPN Communicable DiseasesCynfully SweetNo ratings yet
- Principles of Nursing Documentation PDFDocument33 pagesPrinciples of Nursing Documentation PDFCynfully SweetNo ratings yet
- True Food Consumer Guide: Gmos: Corn-Based ProductsDocument4 pagesTrue Food Consumer Guide: Gmos: Corn-Based ProductsJan BularioNo ratings yet
- Markup0718 410 TDocument8 pagesMarkup0718 410 TCynfully SweetNo ratings yet
- Standard Residential Lease Agreement Version1Document5 pagesStandard Residential Lease Agreement Version1etirosaNo ratings yet
- LEASE BASIC RENTAL AGREEMENT or RESIDENTIAL LEASE This Rental Agreement or Residential Lease Shall Evidence the Complete Terms and Conditions Under Which the Parties Whose Signatures Appear Below Have AgreedDocument4 pagesLEASE BASIC RENTAL AGREEMENT or RESIDENTIAL LEASE This Rental Agreement or Residential Lease Shall Evidence the Complete Terms and Conditions Under Which the Parties Whose Signatures Appear Below Have AgreedJaycee BernardoNo ratings yet
- Markup0718 410 TDocument8 pagesMarkup0718 410 TCynfully SweetNo ratings yet
- I M C I (Imci) : For WHOM?Document8 pagesI M C I (Imci) : For WHOM?Alnair PanisNo ratings yet
- Lease ContractDocument3 pagesLease ContractAR Cuaresma MoralesNo ratings yet
- EPI Care - CHN - Pentagon NotesDocument8 pagesEPI Care - CHN - Pentagon NotesCynfully SweetNo ratings yet
- How To Use The Lens Flares?: Open Your Photoshop ApplicationDocument2 pagesHow To Use The Lens Flares?: Open Your Photoshop ApplicationCynfully SweetNo ratings yet
- Community Organizing in HealthDocument3 pagesCommunity Organizing in HealthNikki Jane Colina PacamarraNo ratings yet
- CHN Module 1Document5 pagesCHN Module 1Cynfully SweetNo ratings yet
- Board Examination Reviewer for Nursing (BERNDocument3 pagesBoard Examination Reviewer for Nursing (BERNCynfully SweetNo ratings yet
- Cocaine's Journey from Medicine to Deadly AddictionDocument6 pagesCocaine's Journey from Medicine to Deadly AddictionDoniele DalorNo ratings yet
- Pathophysiology of FractureDocument2 pagesPathophysiology of FractureEunice CuñadaNo ratings yet
- ITP Explained in Detail - Good OneDocument5 pagesITP Explained in Detail - Good Onemaheshbendigeri5945No ratings yet
- Quarter ApplicationDocument1 pageQuarter ApplicationSouvik DasNo ratings yet
- Diuretics MOA Notes Indications Side Effects DrugsDocument1 pageDiuretics MOA Notes Indications Side Effects Drugsmonica leeNo ratings yet
- Critical Values List: Arterial Blood Gases Test Value CommentsDocument5 pagesCritical Values List: Arterial Blood Gases Test Value CommentsAsepta CecepNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- Escherichia ColiDocument31 pagesEscherichia ColiLizzie Fizzie100% (1)
- BSI MD Ivd Diagnostic Directive Guide Brochure UK enDocument8 pagesBSI MD Ivd Diagnostic Directive Guide Brochure UK enf.baxyNo ratings yet
- Case Study On Prostate CancerDocument16 pagesCase Study On Prostate Cancerferdz02100% (5)
- Kellett - Paranoid Personality Disorder Treatm.Document14 pagesKellett - Paranoid Personality Disorder Treatm.Caramel GazelleNo ratings yet
- Clinical Study of Otomycosis: Fungal Ear Infection Causes, Symptoms & TreatmentDocument16 pagesClinical Study of Otomycosis: Fungal Ear Infection Causes, Symptoms & TreatmentMcraeNo ratings yet
- Cough NCPDocument2 pagesCough NCPMYLENE GRACE ELARCOSANo ratings yet
- Annotated BibDocument19 pagesAnnotated Bibapi-252208553No ratings yet
- Role of orthodontics in TMDDocument19 pagesRole of orthodontics in TMDAngel Rubén Orozco RodríguezNo ratings yet
- Clinical Examinations Crib Sheet v7Document36 pagesClinical Examinations Crib Sheet v7aparish10100% (1)
- The Pocket DoctorDocument132 pagesThe Pocket DoctorArthur Hebert100% (1)
- Dermtimes - Vitiligo Treatment SuccessDocument2 pagesDermtimes - Vitiligo Treatment SuccessradqudahNo ratings yet
- 5 Minute Spotlight - Vacuum Extraction and Forceps DeliveryDocument2 pages5 Minute Spotlight - Vacuum Extraction and Forceps DeliveryMikeNo ratings yet
- Nama ObatDocument13 pagesNama Obatsahmin sahminNo ratings yet
- DAFTAR PUSTAKA ProposalDocument2 pagesDAFTAR PUSTAKA ProposalPipik TaufikNo ratings yet
- Fresenius 2008T Dialysis System - User's Troubleshooting ManualDocument20 pagesFresenius 2008T Dialysis System - User's Troubleshooting ManualCesar AlfaroNo ratings yet
- GI and Liver UWorldDocument5 pagesGI and Liver UWorldCSZNo ratings yet
- History Sales Mei 2020Document16 pagesHistory Sales Mei 2020Daniel Salsha Nophansyah Putra SulaimanNo ratings yet
- Prof J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabweDocument17 pagesProf J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabwedanielNo ratings yet
- Renal PhysiologyDocument5 pagesRenal PhysiologyJayricDepalobosNo ratings yet
- Ethical Issues of Unrelated Hematopoietic Stem Cell Transplantation in Adult Thalassemia PatientsDocument7 pagesEthical Issues of Unrelated Hematopoietic Stem Cell Transplantation in Adult Thalassemia PatientsMcullfy JohnNo ratings yet
- Head Nursing ToolDocument26 pagesHead Nursing ToolJeneva L. LauzonNo ratings yet
- First Generation Anti-Depressants: TCAs and MAOIsDocument54 pagesFirst Generation Anti-Depressants: TCAs and MAOIssangha_mitra_2No ratings yet
- Concept of Pregnancy Final NCM 107 07172019Document6 pagesConcept of Pregnancy Final NCM 107 07172019Jarod Hembrador100% (1)