You might also like
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Gastric Volvulus: Bang Chau, Susan DufelDocument2 pagesGastric Volvulus: Bang Chau, Susan DufelmustikaarumNo ratings yet
- J Epsc 2015 05 012Document4 pagesJ Epsc 2015 05 012Hanung PujanggaNo ratings yet
- Gastric Tuberculosis Mimicking Liver Abscess Ea Case Report: SciencedirectDocument3 pagesGastric Tuberculosis Mimicking Liver Abscess Ea Case Report: SciencedirectJenny Paola RuambaNo ratings yet
- Residents' Clinic: 22-Year-Old Man With Abdominal Pain and RashDocument4 pagesResidents' Clinic: 22-Year-Old Man With Abdominal Pain and RashAkhtar AliNo ratings yet
- Adult Idiopathic Hypertrophic Pyloric Stenosis A Common Presentation With An Uncommon DiagnosisDocument5 pagesAdult Idiopathic Hypertrophic Pyloric Stenosis A Common Presentation With An Uncommon DiagnosiszapomannNo ratings yet
- Jurnal AppendiksDocument6 pagesJurnal AppendiksSiti anasya CahyaNo ratings yet
- Gastritis and Carditis: University of British Columbia, Vancouver, British Columbia, CanadaDocument17 pagesGastritis and Carditis: University of British Columbia, Vancouver, British Columbia, CanadaJose SirittNo ratings yet
- 1 s2.0 S0929644108600089 MainDocument5 pages1 s2.0 S0929644108600089 Maineva kacanjaNo ratings yet
- Eosinophilic Esophagitis in Adults: A Case Series and Literature ReviwDocument6 pagesEosinophilic Esophagitis in Adults: A Case Series and Literature ReviwIJAR JOURNALNo ratings yet
- Gastroesophageal Reflux DiseaseDocument8 pagesGastroesophageal Reflux DiseaseOzzy YunandarNo ratings yet
- Complicated Small-Bowel Diverticulosis: A Case Report and Review of The LiteratureDocument3 pagesComplicated Small-Bowel Diverticulosis: A Case Report and Review of The LiteratureYeudiel SuroNo ratings yet
- 2008 Article BF02993755Document2 pages2008 Article BF02993755Chato Haviz DanayomiNo ratings yet
- Gastroesophageal Reflux DiseaseDocument8 pagesGastroesophageal Reflux Diseasenaufal12345No ratings yet
- Acalasia PDFDocument11 pagesAcalasia PDFJuanita GonzálezNo ratings yet
- Stomach Volvulus: Why Should We Remember It? Case ReviewDocument7 pagesStomach Volvulus: Why Should We Remember It? Case ReviewChristabella Natalia WijayaNo ratings yet
- 3472-2. Manuscript - Word File-25886-1-10-20210921Document1 page3472-2. Manuscript - Word File-25886-1-10-20210921Patricia Peñaflor GrimaldoNo ratings yet
- An Overview of Esophageal Disorders (Nour Al-Huda Hamad's Conflicted Copy 2014-07-19)Document16 pagesAn Overview of Esophageal Disorders (Nour Al-Huda Hamad's Conflicted Copy 2014-07-19)Mysheb SSNo ratings yet
- Dysphagia LusoriaDocument2 pagesDysphagia LusoriaArsha AjNo ratings yet
- Esophageal Disease in Scleroderma: A T: C RDocument7 pagesEsophageal Disease in Scleroderma: A T: C REva OretlaNo ratings yet
- Transition of A Mallory-Weiss Syndrome To A BoerhaDocument5 pagesTransition of A Mallory-Weiss Syndrome To A BoerhaShubhamNo ratings yet
- Case Report: Peritonitis in Patients With Scrub TyphusDocument3 pagesCase Report: Peritonitis in Patients With Scrub TyphusJasleen KaurNo ratings yet
- CT Mesenteroaxial GVDocument6 pagesCT Mesenteroaxial GVkueputuNo ratings yet
- Trilogy of Foregut Midgut and Hindgut Atresias PreDocument5 pagesTrilogy of Foregut Midgut and Hindgut Atresias PreEriekafebriayana RNo ratings yet
- Gastritis Bahasa InggrisDocument7 pagesGastritis Bahasa InggrisNieq Cutex CelaluingindimandjaNo ratings yet
- Gallstone Pancreatitis - CST PDFDocument5 pagesGallstone Pancreatitis - CST PDFDaniel Rosero CadenaNo ratings yet
- Duodenal Ulcer - StatPearls - NCBI BookshelfDocument6 pagesDuodenal Ulcer - StatPearls - NCBI Bookshelfimehap033No ratings yet
- Case GastritisDocument3 pagesCase GastritisMuhammad SyukurNo ratings yet
- Acute Abdomen in Chronic Renal Failure: A. Martinez-Vea, J. Montoliu, C. Monroy, M.Lanuza, J.Lopez Pedret, L. RevertDocument2 pagesAcute Abdomen in Chronic Renal Failure: A. Martinez-Vea, J. Montoliu, C. Monroy, M.Lanuza, J.Lopez Pedret, L. RevertbagussofianNo ratings yet
- Acute Appendicitis in A Patient With Systemic Lupus ErythematosusDocument4 pagesAcute Appendicitis in A Patient With Systemic Lupus ErythematosusJessicaNo ratings yet
- 37poflee EtalDocument3 pages37poflee EtaleditorijmrhsNo ratings yet
- Idiopathic Sclerosing Encapsulating Peritonitis: Abdominal CocoonDocument6 pagesIdiopathic Sclerosing Encapsulating Peritonitis: Abdominal CocoonRameshKumarNo ratings yet
- Gastroenterology Cases PracticeDocument19 pagesGastroenterology Cases PracticeIbtissame BadadNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 pagesIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARINo ratings yet
- Usg Gastritis PDFDocument6 pagesUsg Gastritis PDFtambamanuellaNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- International Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. AwasthiDocument3 pagesInternational Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. Awasthijohanna monsalveNo ratings yet
- Penanganan Terkini Bayi PrematurDocument44 pagesPenanganan Terkini Bayi PrematuryudhagpNo ratings yet
- Achalasia: An Overview of Diagnosis and Treatment: ReviewDocument7 pagesAchalasia: An Overview of Diagnosis and Treatment: ReviewJessica GintingNo ratings yet
- Case 12192Document9 pagesCase 12192Novi OktaviantiNo ratings yet
- International Journal of Health Sciences and Research: Gall Bladder Gangrene and Perforation Complicating Typhoid FeverDocument3 pagesInternational Journal of Health Sciences and Research: Gall Bladder Gangrene and Perforation Complicating Typhoid Feverelsa_imamNo ratings yet
- Peritonitis Following Prepyloric Ulcer Perforation A Case ReportDocument2 pagesPeritonitis Following Prepyloric Ulcer Perforation A Case ReportraysellaNo ratings yet
- Raj KamalDocument5 pagesRaj KamalBhavani Rao ReddiNo ratings yet
- Digestive Endoscopy - 2015 - Ohmiya - Obscure Gastrointestinal Bleeding Diagnosis and TreatmentDocument10 pagesDigestive Endoscopy - 2015 - Ohmiya - Obscure Gastrointestinal Bleeding Diagnosis and Treatmentpgomez156No ratings yet
- Article 1615981002 PDFDocument3 pagesArticle 1615981002 PDFMaria Lyn Ocariza ArandiaNo ratings yet
- Case 16737: Duodenal Atresia in A Fetus With Trisomy 21Document5 pagesCase 16737: Duodenal Atresia in A Fetus With Trisomy 21NasriNo ratings yet
- AppendicitisDocument36 pagesAppendicitisPetro MyronovNo ratings yet
- Esophageal Pneumatosis in The Setting of Small Bowel Ileus With Acute Resolution After Nasogastric Tube DecompressionDocument4 pagesEsophageal Pneumatosis in The Setting of Small Bowel Ileus With Acute Resolution After Nasogastric Tube DecompressionAnggaAdityaNo ratings yet
- Small Bowel Obstruction Due To Phytobezoars: Report of Four Cases and Literature ReviewDocument5 pagesSmall Bowel Obstruction Due To Phytobezoars: Report of Four Cases and Literature ReviewAna Laura Sánchez BaltazarNo ratings yet
- Brede No Ord 2013Document10 pagesBrede No Ord 2013Jonathan ArifputraNo ratings yet
- Gastritis - Facts and Doubts: Original PaperDocument10 pagesGastritis - Facts and Doubts: Original Paperindah setiyaniNo ratings yet
- JGastr10 GERDDocument8 pagesJGastr10 GERDEnderNo ratings yet
- Gastric Volvulus With Hiatal Hernia in A Young Male A Case ReportDocument5 pagesGastric Volvulus With Hiatal Hernia in A Young Male A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Calcagno 2018Document10 pagesCalcagno 2018cut normaya putriNo ratings yet
- Small BowelDocument5 pagesSmall BowelFachry MuhammadNo ratings yet
- Emphysematous Infections of The Abdomen and PelvisDocument19 pagesEmphysematous Infections of The Abdomen and PelvisAle LizárragaNo ratings yet
- EsofagusDocument7 pagesEsofagusWillie VanegasNo ratings yet
- Posterior Perforation of Gastric Ulcer-A Rare Surgical EmergencyDocument7 pagesPosterior Perforation of Gastric Ulcer-A Rare Surgical EmergencyyourinmyheartNo ratings yet
- Paralytic Ileus Complication of Acute Appendicitis Dudley, M.DDocument6 pagesParalytic Ileus Complication of Acute Appendicitis Dudley, M.Dandre nicholasNo ratings yet
- Rekap Pembayaran CBT Osce Ee, Bimbingan & Ukmppd FirstakerDocument2 pagesRekap Pembayaran CBT Osce Ee, Bimbingan & Ukmppd FirstakerNg Chor YaoNo ratings yet
- Logistik Bot 19 Mei 2022 v20220518 v2 - DGN No. Tel-1Document4 pagesLogistik Bot 19 Mei 2022 v20220518 v2 - DGN No. Tel-1Ng Chor YaoNo ratings yet
- Cakes: Red Velvet Cake Ube Velvet CakeDocument3 pagesCakes: Red Velvet Cake Ube Velvet CakeNg Chor YaoNo ratings yet
- Golf Bandar Kemayoran Membership Fee 2020Document1 pageGolf Bandar Kemayoran Membership Fee 2020Ng Chor YaoNo ratings yet
- HBV DecisionMaking Jan2015 WEBDocument2 pagesHBV DecisionMaking Jan2015 WEBNg Chor YaoNo ratings yet
- Stase 21 Oktober 2019Document17 pagesStase 21 Oktober 2019Ng Chor YaoNo ratings yet
- Stase 16 September 2019Document18 pagesStase 16 September 2019Ng Chor YaoNo ratings yet
- Stase 16 September 2019Document18 pagesStase 16 September 2019Ng Chor YaoNo ratings yet
- Nab Kurikulum09 Blok24Document5 pagesNab Kurikulum09 Blok24Ng Chor YaoNo ratings yet
- Stase 23 September 2019Document6 pagesStase 23 September 2019Ng Chor YaoNo ratings yet
- Nilai Integrasi 1 Blok 26 SEMESTER GENAP 2018/2019: NO NIM Nama JLH Benar JLH Salah NilaiDocument4 pagesNilai Integrasi 1 Blok 26 SEMESTER GENAP 2018/2019: NO NIM Nama JLH Benar JLH Salah NilaiNg Chor YaoNo ratings yet
- Indigenous Therapies - Sleep and WorkDocument13 pagesIndigenous Therapies - Sleep and WorkRaabiyaNo ratings yet
- Amlodipine in HypertensionDocument12 pagesAmlodipine in HypertensionDinny Novia WNo ratings yet
- Differential Diagnosis of Cervicobrachial PainDocument11 pagesDifferential Diagnosis of Cervicobrachial PainpuchioNo ratings yet
- JOGCan 2018 Fetal Surveillance B IntrapartumDocument25 pagesJOGCan 2018 Fetal Surveillance B IntrapartumMiguel Guillermo Salazar ClavijoNo ratings yet
- BACHELOR IN NURSING - Docx (Reflection)Document9 pagesBACHELOR IN NURSING - Docx (Reflection)siti husniNo ratings yet
- Cereves Psqi EngDocument6 pagesCereves Psqi EngMégane ErblangNo ratings yet
- Training in Clinical RadiologyDocument12 pagesTraining in Clinical RadiologyAnoop TitusNo ratings yet
- Republic Polytechnic: Consent FormDocument4 pagesRepublic Polytechnic: Consent FormmegNo ratings yet
- Improving The Physical Health of People With Mental Health ProblemsDocument61 pagesImproving The Physical Health of People With Mental Health ProblemsThierry UhawenimanaNo ratings yet
- Basic 7 Music 1ST Term E-NotesDocument16 pagesBasic 7 Music 1ST Term E-Notessamuel joshuaNo ratings yet
- GAD Accomplishment Report 2021Document16 pagesGAD Accomplishment Report 2021Edgar Sanchez EndozoNo ratings yet
- FeversDocument2 pagesFeversMiranda Castro HomeopathyNo ratings yet
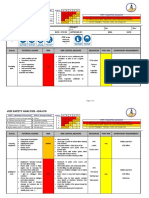
- JSA For Coating and Raping Activity in TankDocument7 pagesJSA For Coating and Raping Activity in TankEslam lotfy- Eslam elsadatNo ratings yet
- 2016 Physical Fitness TestDocument13 pages2016 Physical Fitness TestDafchen Nio MahasolNo ratings yet
- New India - OMP For StudentsDocument11 pagesNew India - OMP For Studentsshreeket3953No ratings yet
- Torreon - Ge - STS - Group 37 - MidtermDocument8 pagesTorreon - Ge - STS - Group 37 - MidtermMary Jean TorreonNo ratings yet
- Goiter Golezgwaponacute2Document3 pagesGoiter Golezgwaponacute2Julie Ann Tejadillo FullanteNo ratings yet
- Challenged ChildDocument30 pagesChallenged ChildkrishnasreeNo ratings yet
- Vitamins Key To Correction Biochemistry Final ExamsDocument3 pagesVitamins Key To Correction Biochemistry Final Examspflorendo_1No ratings yet
- 2 For Counselling Workshop (Revised)Document18 pages2 For Counselling Workshop (Revised)Debapriya MukherjeeNo ratings yet
- Seerat Kaur - FEMALE - 22 Yrs +918968148007 APJ1.0020209332 5801854Document2 pagesSeerat Kaur - FEMALE - 22 Yrs +918968148007 APJ1.0020209332 5801854Seerat KaurNo ratings yet
- Microcurrent Instructions PDFDocument11 pagesMicrocurrent Instructions PDFFuh Ken Chin100% (1)
- JSA-018 Lifting With Mobile CraneDocument5 pagesJSA-018 Lifting With Mobile CraneOmar Dhieb100% (1)
- 09 Health Worksheet English MediumDocument90 pages09 Health Worksheet English Mediumnadhanisthar100% (1)
- RamzanDocument8 pagesRamzanapi-552311432No ratings yet
- Teens Lead Very Stressful LivesDocument1 pageTeens Lead Very Stressful LivesIAMANDI MARINA-CAMELIANo ratings yet
- DelysidDocument2 pagesDelysidAlexandru CotrutaNo ratings yet
- Quiz Comprehension and Error Identification W2Document3 pagesQuiz Comprehension and Error Identification W2norlianaNo ratings yet
- Health Psychology TestDocument19 pagesHealth Psychology TestjosephNo ratings yet
- Superlife PresentationDocument3 pagesSuperlife PresentationSalami FahidatNo ratings yet