You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- How To Manage Heart Failure in Primary Health Care Prof. Djoko Soemantri MD FIHADocument43 pagesHow To Manage Heart Failure in Primary Health Care Prof. Djoko Soemantri MD FIHAIvor Wilopo100% (1)
- Prevalence of Overweight and Obesity Among Medical College Students, BengaluruDocument6 pagesPrevalence of Overweight and Obesity Among Medical College Students, BengaluruTri UtomoNo ratings yet
- The Association Between LungDocument3 pagesThe Association Between LungTri UtomoNo ratings yet
- College Students Eating Habits and Knowledge of Nutritional RequirementsDocument5 pagesCollege Students Eating Habits and Knowledge of Nutritional RequirementsTri UtomoNo ratings yet
- Dietary Patterns and Overweight/Obesity: A Review ArticleDocument8 pagesDietary Patterns and Overweight/Obesity: A Review ArticleTri UtomoNo ratings yet
- DR - Jetty - Executive Summary of Perioperative ManagementDocument28 pagesDR - Jetty - Executive Summary of Perioperative ManagementDilaNo ratings yet
- Dr. Cholid - Lifestyle Management Update in CardiovascularDocument26 pagesDr. Cholid - Lifestyle Management Update in CardiovascularHadiyana Arief HafizNo ratings yet
- FFN GuidelineDocument13 pagesFFN GuidelineTri UtomoNo ratings yet
- Efficacy and Safety of Recombinant Human Parathyroid Hormone in HypoparathyriodismDocument9 pagesEfficacy and Safety of Recombinant Human Parathyroid Hormone in HypoparathyriodismTri UtomoNo ratings yet
- Novel Subgroups of Adult-Onset Diabetes and Their AssociationDocument9 pagesNovel Subgroups of Adult-Onset Diabetes and Their AssociationTri UtomoNo ratings yet
- 25 Patofisiologi EpilepsiDocument13 pages25 Patofisiologi EpilepsiWisnuBaskoroNo ratings yet
- Associations of HIV InfectionDocument7 pagesAssociations of HIV InfectionTri UtomoNo ratings yet
- AdvBiomedRes7158-3967164 110111Document6 pagesAdvBiomedRes7158-3967164 110111Tri UtomoNo ratings yet
- Study of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsDocument4 pagesStudy of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsTri UtomoNo ratings yet
- Aspirin and Extended-Release DipyridamoleDocument14 pagesAspirin and Extended-Release DipyridamoleTri UtomoNo ratings yet
- Hosts UmbrellaDocument1 pageHosts UmbrellaFabsor SoralNo ratings yet
- Use of S-LANSS Tool to Predict PHNDocument8 pagesUse of S-LANSS Tool to Predict PHNTri UtomoNo ratings yet
- Treatment of Acute PDFDocument22 pagesTreatment of Acute PDFTri UtomoNo ratings yet
- Journal 4 Nejmoa1215340 NeuroDocument9 pagesJournal 4 Nejmoa1215340 NeuroDyo O RNo ratings yet
- Statins and The Risk of Herpes ZosterDocument7 pagesStatins and The Risk of Herpes ZosterTri UtomoNo ratings yet
- High On Treatment Platelet Reactivity To Aspirin and Clopidogrel inDocument23 pagesHigh On Treatment Platelet Reactivity To Aspirin and Clopidogrel inTri UtomoNo ratings yet
- Hypovolemic ShockDocument2 pagesHypovolemic ShockTri UtomoNo ratings yet
- Identification of The Severe Sepsis Patient at TriageDocument27 pagesIdentification of The Severe Sepsis Patient at TriageTri UtomoNo ratings yet
- Circulatory ShockDocument9 pagesCirculatory ShockTri UtomoNo ratings yet
- Dehidrasi Dan SyokDocument4 pagesDehidrasi Dan SyokBilly Shan LastKagerooboro0% (1)
- The Role of RegionalDocument5 pagesThe Role of RegionalTri UtomoNo ratings yet
- Neurointerventionist Vol 3 No 1.edinburgh.: Daftar PustakaDocument3 pagesNeurointerventionist Vol 3 No 1.edinburgh.: Daftar PustakaAnonymous F3PADS0xGNo ratings yet
- General Anaesthesia ForDocument4 pagesGeneral Anaesthesia ForTri UtomoNo ratings yet
- Cognitive Correlates in Amyotrophic Lateral SclerosisDocument8 pagesCognitive Correlates in Amyotrophic Lateral SclerosisTri UtomoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Midterm Examination in PRINCIPLES OF MARKETINGDocument2 pagesMidterm Examination in PRINCIPLES OF MARKETINGGlyzel Ann Damicog GarciaNo ratings yet
- Warwick Dissertation TemplateDocument7 pagesWarwick Dissertation TemplateWriteMyPaperCollegeSingapore100% (1)
- Metallurgical Condition AssessmentDocument2 pagesMetallurgical Condition AssessmentJohnNo ratings yet
- Project Riske ManagementDocument7 pagesProject Riske ManagementMohammed Lawal AhmedNo ratings yet
- Study On Perfromance Appraisal System in HPCLDocument12 pagesStudy On Perfromance Appraisal System in HPCLomkinggNo ratings yet
- Report Writing Guide: 10 Easy StepsDocument19 pagesReport Writing Guide: 10 Easy StepsAhmad ButtNo ratings yet
- Bloomberg Politics National Poll - v3 - Nov. 18, 2015Document4 pagesBloomberg Politics National Poll - v3 - Nov. 18, 2015Bloomberg PoliticsNo ratings yet
- Marketing Research: DR - Kalpana AgrawalDocument15 pagesMarketing Research: DR - Kalpana Agrawalkalpna_prestigeNo ratings yet
- Project QuestionnaireDocument4 pagesProject QuestionnaireMufidul HassanNo ratings yet
- Lesson Plan CritiqueDocument3 pagesLesson Plan Critiqueapi-357257220No ratings yet
- A Physical Self-Efficacy Scale For Children2008Document9 pagesA Physical Self-Efficacy Scale For Children2008tmilic6No ratings yet
- Research Paper Best TitleDocument4 pagesResearch Paper Best Titlepoypdibkf100% (1)
- CIH Candidate Handbook Guide to Becoming CertifiedDocument21 pagesCIH Candidate Handbook Guide to Becoming CertifiedHalim HasanNo ratings yet
- Literature Review: Naresh T Chauhan Community Medicine Deptt, Government Medical College, SuratDocument39 pagesLiterature Review: Naresh T Chauhan Community Medicine Deptt, Government Medical College, SuratdrnareshchauhanNo ratings yet
- Araujo 2016Document14 pagesAraujo 2016NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Best Thesis TitlesDocument7 pagesBest Thesis Titlesbseb81xq100% (1)
- 2006-11-13 (Employability - KSR College)Document26 pages2006-11-13 (Employability - KSR College)Krishnamurthy Prabhakar100% (2)
- Asset-liability gap analysis of Indian banksDocument8 pagesAsset-liability gap analysis of Indian banksTelika RamuNo ratings yet
- Preparing Children To Solve ProblemsDocument31 pagesPreparing Children To Solve ProblemsJennylyn Layan AlnajesNo ratings yet
- DISS 16th Applications and Intersections of The Approaches in Addressing Social ProblemsDocument6 pagesDISS 16th Applications and Intersections of The Approaches in Addressing Social ProblemsChristine Elisa D. Durano69% (13)
- Biomedical EngineeringDocument12 pagesBiomedical EngineeringBiomedical Engineering100% (1)
- Appendix A: Textual Variants of Cloud AtlasDocument30 pagesAppendix A: Textual Variants of Cloud AtlasRosemary SmithNo ratings yet
- Guidelines For The Medicines and Therapeutics CommitteeDocument20 pagesGuidelines For The Medicines and Therapeutics CommitteeLorezza Miranda Aguilar100% (1)
- Elementary StatDocument15 pagesElementary StatGeralyn T. FamilganNo ratings yet
- Legal Internship Resume - Sample 1: Sachin XXXXXXDocument4 pagesLegal Internship Resume - Sample 1: Sachin XXXXXXshivani soniNo ratings yet
- Obstruction. Return of Bowel Sounds - Not Effective To Judges Post Op IleusDocument6 pagesObstruction. Return of Bowel Sounds - Not Effective To Judges Post Op Ileusjustin_saneNo ratings yet
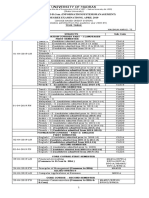
- University of Madras BSc ISM BCom ISM degree exams timetable April 2019Document14 pagesUniversity of Madras BSc ISM BCom ISM degree exams timetable April 2019RoshniNo ratings yet
- Efficacy of EUS-RFA in Pancreatic Tumors: Is It Ready For Prime Time? A Systematic Review and Meta-AnalysisDocument9 pagesEfficacy of EUS-RFA in Pancreatic Tumors: Is It Ready For Prime Time? A Systematic Review and Meta-AnalysisRadinal MauludiNo ratings yet
- Factors Influencing STEM Students' Performance in CalculusDocument73 pagesFactors Influencing STEM Students' Performance in CalculusDana NicoleNo ratings yet
- Edtpa Secondary History-Social Studies - Planning Commentary JB Final 1Document7 pagesEdtpa Secondary History-Social Studies - Planning Commentary JB Final 1api-34774774075% (4)