You might also like
- Coagulation DrugsDocument1 pageCoagulation Drugsmed testNo ratings yet
- Ninja - Antihyperlipidemics PDFDocument3 pagesNinja - Antihyperlipidemics PDFErica Hyeyeon Lee100% (1)
- Test LFTsDocument2 pagesTest LFTsostarburstoNo ratings yet
- Ninja - Antianginal Drugs PDFDocument2 pagesNinja - Antianginal Drugs PDFErica Hyeyeon LeeNo ratings yet
- Ninja - Anemias PDFDocument1 pageNinja - Anemias PDFErica Hyeyeon LeeNo ratings yet
- Chart - WBC DisordersDocument1 pageChart - WBC DisordersSamuel RothschildNo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
- Antibiotics Chart 1Document7 pagesAntibiotics Chart 1Vee MendNo ratings yet
- Anemia Flow ChartDocument1 pageAnemia Flow ChartCynthiaNo ratings yet
- NSAIDS and SteroidsDocument2 pagesNSAIDS and Steroidsmed testNo ratings yet
- Pharm Expansion 17 NDFDocument1 pagePharm Expansion 17 NDFNokz M. Raki-inNo ratings yet
- Glomerulonephritis Cheat Sheet PDFDocument1 pageGlomerulonephritis Cheat Sheet PDFAnonymous aA9Ol6239No ratings yet
- Tumor Markers: Blood Group AntigenDocument5 pagesTumor Markers: Blood Group AntigenAngela ReyesNo ratings yet
- AntimicrobialsDocument1 pageAntimicrobialsRomaine Barrett100% (1)
- Semester 2 Drug ListDocument7 pagesSemester 2 Drug ListNam_Pham_6481No ratings yet
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDocument4 pagesLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testNo ratings yet
- Drug TerminologyDocument5 pagesDrug Terminologyimdaking123No ratings yet
- Renal Chart 2Document21 pagesRenal Chart 2fortheloveofmedicineNo ratings yet
- (CV2) Pharmacology of AnticoagulantsDocument6 pages(CV2) Pharmacology of AnticoagulantsHanifa Shereen B. AliNo ratings yet
- DDX Gastrointestinal Disorders ChartDocument20 pagesDDX Gastrointestinal Disorders ChartDavid UribeNo ratings yet
- Pharmacology Main DrugsDocument14 pagesPharmacology Main DrugsSabir KhanNo ratings yet
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Laboratory Reference RangesDocument12 pagesLaboratory Reference RangesPrashanth Raju100% (1)
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocument8 pagesApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuNo ratings yet
- Hierarchy of O2 Delivery SystemsDocument1 pageHierarchy of O2 Delivery SystemsRevNo ratings yet
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocument5 pagesPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNo ratings yet
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezNo ratings yet
- Decreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisDocument8 pagesDecreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisSamuel RothschildNo ratings yet
- Biochemisty Cheat SheetsDocument4 pagesBiochemisty Cheat SheetsNatalie KingNo ratings yet
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDocument26 pagesA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- Role of Drugs That Affect Renin Angiotensin SystemDocument22 pagesRole of Drugs That Affect Renin Angiotensin Systemash ashNo ratings yet
- Anticoagulation Care GuideDocument13 pagesAnticoagulation Care GuideSadiah Hasyim AlweiniNo ratings yet
- Lab Values and Vital SignsDocument4 pagesLab Values and Vital SignsWole Olaluwoye100% (1)
- Acid BaseDocument89 pagesAcid BaseEdouinaNo ratings yet
- 0.5. ANS Quicksheet PDFDocument1 page0.5. ANS Quicksheet PDFErica Hyeyeon LeeNo ratings yet
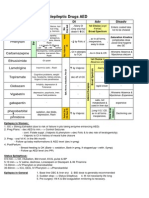
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Opioids PDFDocument2 pagesOpioids PDFErica Hyeyeon LeeNo ratings yet
- Drugs in Blood DisordersDocument1 pageDrugs in Blood DisordersSantosh patelNo ratings yet
- Drug Compatibility in Intravenous Y-Site AdministrationDocument4 pagesDrug Compatibility in Intravenous Y-Site Administrationtuti haryatiNo ratings yet
- Internal Medicine #1Document167 pagesInternal Medicine #1Nikhil RayarakulaNo ratings yet
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- Notes: Bernard-Soulier Syndrome (BSS)Document3 pagesNotes: Bernard-Soulier Syndrome (BSS)Himalaya AggarwalNo ratings yet
- Common Prefixes and SuffixesDocument5 pagesCommon Prefixes and Suffixestriddle1969100% (1)
- Thyroid Gland: Sheena Mae SangutanDocument27 pagesThyroid Gland: Sheena Mae SangutanMarrah Avila Acuin100% (1)
- Breast CancerDocument6 pagesBreast Cancersarguss14No ratings yet
- Abdo Exam TableDocument2 pagesAbdo Exam Tableapi-195986134No ratings yet
- Oncologic EmergenciesDocument3 pagesOncologic EmergenciesMiguel Cuevas DolotNo ratings yet
- UrinalysisDocument9 pagesUrinalysisSukma EffendyNo ratings yet
- PG PREPARATION - Mnemonics in PharmacologyDocument12 pagesPG PREPARATION - Mnemonics in PharmacologyRaveen KumarNo ratings yet
- Abx FinalDocument3 pagesAbx Finalyanks1120No ratings yet
- Electrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionDocument6 pagesElectrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionmkninnyNo ratings yet
- Mnemonic SDocument42 pagesMnemonic SWen Jie LauNo ratings yet
- First Aid PharmacoDocument61 pagesFirst Aid PharmacogirNo ratings yet
- Antibiotics and MnemonicsDocument8 pagesAntibiotics and MnemonicsMichael Howes100% (1)
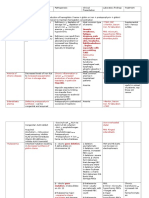
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Clinical Medicine - Lecture: - Topic: - DateDocument3 pagesClinical Medicine - Lecture: - Topic: - DateqselmmNo ratings yet
- Disorders of The BoneDocument2 pagesDisorders of The BoneRPh Krishna Chandra JagritNo ratings yet
- منار كمDocument61 pagesمنار كمFemale calmNo ratings yet
- L P 4 Blood Pharmacology - Final-2022Document26 pagesL P 4 Blood Pharmacology - Final-2022Zakria Al-HadadNo ratings yet
- Immunopharmacology PDFDocument2 pagesImmunopharmacology PDFErica Hyeyeon LeeNo ratings yet
- GI Drugs PDFDocument6 pagesGI Drugs PDFErica Hyeyeon Lee100% (1)
- Pharmacogenomics PDFDocument1 pagePharmacogenomics PDFErica Hyeyeon LeeNo ratings yet
- Opioids PDFDocument2 pagesOpioids PDFErica Hyeyeon LeeNo ratings yet
- Nsaids: Celecoxib, Meloxicam Aspirin, Diclofenac, Ibuprofen, Indomethacin Ketorolac, Naproxen, PiroxicamDocument2 pagesNsaids: Celecoxib, Meloxicam Aspirin, Diclofenac, Ibuprofen, Indomethacin Ketorolac, Naproxen, PiroxicamErica Hyeyeon LeeNo ratings yet
- Asthma - Respiratory PDFDocument1 pageAsthma - Respiratory PDFErica Hyeyeon Lee0% (1)
- Ninja - Antiarrhythmic Drugs PDFDocument7 pagesNinja - Antiarrhythmic Drugs PDFErica Hyeyeon Lee100% (1)
- Ninja - Drugs Heart Failure PDFDocument4 pagesNinja - Drugs Heart Failure PDFErica Hyeyeon LeeNo ratings yet
- Ninja - Adrenergic Drugs PDFDocument6 pagesNinja - Adrenergic Drugs PDFErica Hyeyeon Lee100% (1)
- Ninja - Anti-HTN PDFDocument6 pagesNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Ninja - Diuretics PDFDocument3 pagesNinja - Diuretics PDFErica Hyeyeon Lee100% (1)
- Ninja - Autacoids PDFDocument3 pagesNinja - Autacoids PDFErica Hyeyeon LeeNo ratings yet
- Pharmacokinetics - Introduction To ANS PDFDocument2 pagesPharmacokinetics - Introduction To ANS PDFErica Hyeyeon Lee100% (1)
- Ninja - Cholinergic Drugs PDFDocument4 pagesNinja - Cholinergic Drugs PDFErica Hyeyeon Lee100% (2)
- 0.5. ANS Quicksheet PDFDocument1 page0.5. ANS Quicksheet PDFErica Hyeyeon LeeNo ratings yet
- What Is Health EconomicDocument8 pagesWhat Is Health Economicbacky_pzNo ratings yet
- 04 GTTDocument15 pages04 GTTAshish TuraleNo ratings yet
- Impaired Oral Mucous Membranes - NCPDocument2 pagesImpaired Oral Mucous Membranes - NCPXtianna Jade Doquila100% (1)
- Pacu Cover LetterDocument6 pagesPacu Cover Letterbcr9srp4100% (2)
- Eczema and DermatitisDocument7 pagesEczema and DermatitisDian BaldonadoNo ratings yet
- Ventilator Intensive CareDocument1 pageVentilator Intensive CareMuhammad Abdullah ButtNo ratings yet
- Research Article 1Document13 pagesResearch Article 1Nicole BamentNo ratings yet
- Philhealth TB PDFDocument35 pagesPhilhealth TB PDFO.r. CadzNo ratings yet
- 11 Questions To Help You Make Sense of A Trial: How To Use This Appraisal ToolDocument6 pages11 Questions To Help You Make Sense of A Trial: How To Use This Appraisal ToolmailcdgnNo ratings yet
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument19 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- CATHETERIZATIONDocument13 pagesCATHETERIZATIONSarah Uy Caronan100% (1)
- Arterial Blood GasDocument55 pagesArterial Blood GasRathis Dasan100% (1)
- Understanding and Using Namcs and Nhamcs DataDocument25 pagesUnderstanding and Using Namcs and Nhamcs Dataanu riazNo ratings yet
- Patient Safety Full ReportDocument40 pagesPatient Safety Full ReportYudi Ariesta Chandra100% (1)
- ECGDocument154 pagesECGSandeep BansalNo ratings yet
- Death by Modern MedicineDocument3 pagesDeath by Modern MedicineAes_Sedai50% (2)
- Neurological Basis of BehaviorDocument31 pagesNeurological Basis of BehaviorAqsa MurtazaNo ratings yet
- Journal Reading - Myringitis - Elisabeth PattyDocument14 pagesJournal Reading - Myringitis - Elisabeth PattyLipatOla123No ratings yet
- Transport of Sick NB PDFDocument25 pagesTransport of Sick NB PDFirene aurelia100% (1)
- Aseptic Techniques Operating RoomDocument12 pagesAseptic Techniques Operating RoomCyril CauilanNo ratings yet
- Perdarahan Saluran Cerna Atas Dan BawahDocument34 pagesPerdarahan Saluran Cerna Atas Dan BawahKharisma PrabowoNo ratings yet
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- PeritonitisDocument21 pagesPeritonitischrisyenNo ratings yet
- Aun Perfusor FM - User ManualDocument20 pagesAun Perfusor FM - User ManualBayani JuanNo ratings yet
- Diagnostic Evaluation and Management of The Solitary Pulmonary NoduleDocument21 pagesDiagnostic Evaluation and Management of The Solitary Pulmonary NoduleGonzalo Leal100% (1)
- Ms Emergency Disaster Preparedness-J11-212 UpdtdDocument5 pagesMs Emergency Disaster Preparedness-J11-212 UpdtdyusiviNo ratings yet
- Combination SyndromeDocument9 pagesCombination SyndromeAmar BimavarapuNo ratings yet
- Promoting Health - Sample ChapterDocument14 pagesPromoting Health - Sample Chapterricardo4emeiaNo ratings yet
- English 112 Performance TaskDocument2 pagesEnglish 112 Performance TaskJohn Benedict VocalesNo ratings yet
- Mascc Antiemetic Guidelines English v.1.2.1Document55 pagesMascc Antiemetic Guidelines English v.1.2.1cricriNo ratings yet