You might also like
- Seven Habits of Highly Effective PeopleDocument4 pagesSeven Habits of Highly Effective PeopleJayesh JainNo ratings yet
- Darden ResumesDocument87 pagesDarden Resumescyberdevil321No ratings yet
- 30 60 90 Day Plan SummaryDocument6 pages30 60 90 Day Plan SummaryAllen Kyn Bacolod Bunda100% (4)
- Refrigerating Machine Operator: Passbooks Study GuideFrom EverandRefrigerating Machine Operator: Passbooks Study GuideNo ratings yet
- MHNDocument6 pagesMHNParameshNavileNo ratings yet
- Internship Waiver FormDocument4 pagesInternship Waiver FormAngela TabudlongNo ratings yet
- Permit To Study PDFDocument2 pagesPermit To Study PDFbrokett23No ratings yet
- Paper Airplane ActivityDocument4 pagesPaper Airplane ActivityRey AbarientosNo ratings yet
- ROTC Student Module 1 (Ver2020)Document51 pagesROTC Student Module 1 (Ver2020)Albert Añasco60% (5)
- Good Math Lesson PlansDocument36 pagesGood Math Lesson PlansZulsubhaDaniSiti100% (1)
- BrandPRO Summary PDFDocument2 pagesBrandPRO Summary PDFBishruta BanerjeeNo ratings yet
- Improving Students' Reading Comprehension through Action ResearchDocument91 pagesImproving Students' Reading Comprehension through Action ResearchClaire CabactulanNo ratings yet
- University of Southeastern PhilippinesDocument11 pagesUniversity of Southeastern PhilippinesShin BusqueNo ratings yet
- Main Documents of Mba SipDocument13 pagesMain Documents of Mba SipShashank MishraNo ratings yet
- SIP Documents 2022Document17 pagesSIP Documents 2022Entertainment ki lifeNo ratings yet
- Internship Regulations for Engineering CoursesDocument6 pagesInternship Regulations for Engineering CoursesMostafa Ayman Mohammed NageebNo ratings yet
- Placement Agreement Form: 1. Student InformationDocument3 pagesPlacement Agreement Form: 1. Student InformationSteeve GaspardNo ratings yet
- Industrial Training Diary: Sri Balaji College of Engineering and TechnologyDocument7 pagesIndustrial Training Diary: Sri Balaji College of Engineering and TechnologyshubhNo ratings yet
- Summer Training Report on Web DevelopmentDocument14 pagesSummer Training Report on Web DevelopmentROHIT HANSALIYANo ratings yet
- Manit PHD FormDocument5 pagesManit PHD Formakchourasia709No ratings yet
- On - The - Job Training 2: Southern Luzon State University Tiaong CampusDocument9 pagesOn - The - Job Training 2: Southern Luzon State University Tiaong CampusJp Isles MagcawasNo ratings yet
- PHD FormDocument2 pagesPHD FormMAX PAYNENo ratings yet
- Undertaking For Attendance SuDocument1 pageUndertaking For Attendance SushubhamNo ratings yet
- Industrial Training Logbook UiTMNS FSKM MAC 2021Document27 pagesIndustrial Training Logbook UiTMNS FSKM MAC 2021Faiz AmiruddinNo ratings yet
- PHD - MDocument2 pagesPHD - MShalini AruneshNo ratings yet
- Guidelines For Summer TrainingDocument3 pagesGuidelines For Summer TrainingAshish SanghaviNo ratings yet
- Application Form Goa University Teaching PositionsDocument16 pagesApplication Form Goa University Teaching PositionsrajaperumalNo ratings yet
- Practicum Form Mid Year Summer 2021Document22 pagesPracticum Form Mid Year Summer 2021Jayson GamoNo ratings yet
- PHD Form July2012 2Document9 pagesPHD Form July2012 2Malik MalikNo ratings yet
- Course Enrolment FormDocument3 pagesCourse Enrolment FormMilos ZivkovicNo ratings yet
- Form 4: Transcript Request: For Institute Use OnlyDocument1 pageForm 4: Transcript Request: For Institute Use OnlyasdasNo ratings yet
- Academic and Financial Acceptance 20201027Document1 pageAcademic and Financial Acceptance 20201027Sb thangNo ratings yet
- Certificate FormatsDocument12 pagesCertificate FormatsrajkalamaeroNo ratings yet
- Jodhpur National University application formDocument3 pagesJodhpur National University application formsidharth kumarNo ratings yet
- Malaviya National Institute of Technology: Placement & Training CellDocument2 pagesMalaviya National Institute of Technology: Placement & Training CellAshutosh RaiNo ratings yet
- Admission Brochure for Post Graduate Technical CoursesDocument1 pageAdmission Brochure for Post Graduate Technical CoursesAshutosh ShuklaNo ratings yet
- Attested Copy of Past Port Size Photo Pasted HereDocument5 pagesAttested Copy of Past Port Size Photo Pasted HerePragyan SenNo ratings yet
- Mandatory Summer Training FormatDocument2 pagesMandatory Summer Training FormatMAYANK AGRAWALNo ratings yet
- LOG BOOK Soft Copy'Document15 pagesLOG BOOK Soft Copy'Emy Kamal100% (3)
- Apprenticeship Contract FormDocument8 pagesApprenticeship Contract FormThabo Allie LetshwitiNo ratings yet
- HNBGU Professor Associate Professor Notification Http://jobnotificationsbysms - Blogspot.comDocument7 pagesHNBGU Professor Associate Professor Notification Http://jobnotificationsbysms - Blogspot.comUdyoga VartamanamuNo ratings yet
- Registration Form PlacementDocument2 pagesRegistration Form PlacementGurpreet SharmaNo ratings yet
- BUAS SWS Application Academic Leave V5Document2 pagesBUAS SWS Application Academic Leave V5Manjesh RNo ratings yet
- Application Form For PEC, PUDocument2 pagesApplication Form For PEC, PURaghu Veer PushadapuNo ratings yet
- Application FormxcvDocument5 pagesApplication Formxcvbalamurugan_S1985No ratings yet
- Students Undertaking For Participating Placement ActivityDocument2 pagesStudents Undertaking For Participating Placement ActivityShubham DamaniaNo ratings yet
- Application for Permission to StudyDocument2 pagesApplication for Permission to StudyNewgleer WengNo ratings yet
- Annexure-I Nomination/Registration Form - Applicants of Indian NationalityDocument8 pagesAnnexure-I Nomination/Registration Form - Applicants of Indian NationalityRohitNo ratings yet
- MOU-OJT SampleDocument3 pagesMOU-OJT SampleyanobrutasNo ratings yet
- CIPET Admission UndertakingDocument10 pagesCIPET Admission UndertakingMani KantaNo ratings yet
- University of Sindh: Directorate of Research and Graduate StudiesDocument2 pagesUniversity of Sindh: Directorate of Research and Graduate StudiesShehzad KhanNo ratings yet
- 05 NFP Undertaking For Internship v2010Document2 pages05 NFP Undertaking For Internship v2010aman_jain_52No ratings yet
- Student Requirements v1Document23 pagesStudent Requirements v1Arianne CondezNo ratings yet
- MNIT Jaipur student summer training requestDocument2 pagesMNIT Jaipur student summer training requestAbhishek AgarwalNo ratings yet
- South Delhi Polytechnic admission formsDocument2 pagesSouth Delhi Polytechnic admission formsAnonymous 0wXXmp1No ratings yet
- Tutor FormDocument6 pagesTutor FormAsnan Habib SaniNo ratings yet
- Ceat Ip FormsDocument5 pagesCeat Ip FormsPatricia DellabanNo ratings yet
- OJT FormDocument7 pagesOJT FormRosecel Jayson Romano RicoNo ratings yet
- Training Memorandum of Agreement/Waiver: Polytechnic University of The Philippines Quezon City BranchDocument3 pagesTraining Memorandum of Agreement/Waiver: Polytechnic University of The Philippines Quezon City BranchAnton ArponNo ratings yet
- College of Engineering and Technology: 1. Personal DetailsDocument6 pagesCollege of Engineering and Technology: 1. Personal DetailskrishnandrkNo ratings yet
- Rules & Regulations Placement PrintoutDocument1 pageRules & Regulations Placement PrintoutAnkur ApteNo ratings yet
- Acgcet 2018 Regis FormDocument1 pageAcgcet 2018 Regis FormSivaganesh SelvarajNo ratings yet
- Indirect Taxes Internship Scheme, 2023Document3 pagesIndirect Taxes Internship Scheme, 2023Ayushman PatnaikNo ratings yet
- Myfile APPLICATION FORM FOR SRLUDocument2 pagesMyfile APPLICATION FORM FOR SRLUIshtiyak KhanNo ratings yet
- Department of Education Division of City Schools Application For Permission To StudyDocument2 pagesDepartment of Education Division of City Schools Application For Permission To StudyJonas Miranda CabusbusanNo ratings yet
- Assistant Professor Application & DetailsDocument5 pagesAssistant Professor Application & DetailsJayapal RajanNo ratings yet
- AbstractDocument8 pagesAbstractgauravNo ratings yet
- Application for Permission to Study Outside SchoolDocument2 pagesApplication for Permission to Study Outside Schoolclaire juarezNo ratings yet
- 2023 Logbook Format - Weekly - SimplifiedDocument15 pages2023 Logbook Format - Weekly - Simplifiedorvyucsi 2221No ratings yet
- David Hartman InterviewDocument7 pagesDavid Hartman Interviewapi-303140970No ratings yet
- Math g4 m4 Topic A OverviewDocument2 pagesMath g4 m4 Topic A OverviewzeynepNo ratings yet
- HRM Core Activities ScribdDocument5 pagesHRM Core Activities Scribdmatildabeecher3605No ratings yet
- BBA Curriculum Guide 2022-23Document10 pagesBBA Curriculum Guide 2022-23Geeta UnivNo ratings yet
- Cultural TranslationDocument16 pagesCultural Translationsaeedalimi0% (1)
- Eng8 WLP Q3 Week3Document3 pagesEng8 WLP Q3 Week3ANNABEL PALMARINNo ratings yet
- Maimonides' Middle Way: Teleology As A Guide For The PerplexedDocument22 pagesMaimonides' Middle Way: Teleology As A Guide For The PerplexedgipecNo ratings yet
- Caregiving Las Week 2Document16 pagesCaregiving Las Week 2Florame OñateNo ratings yet
- All Saints Catholic College Specialist in Humanities: Year 11 InformationDocument2 pagesAll Saints Catholic College Specialist in Humanities: Year 11 Informationjanrocks1No ratings yet
- Pumpkin LessonDocument5 pagesPumpkin Lessonapi-284900448No ratings yet
- ACIO Grade II exam questions and answersDocument34 pagesACIO Grade II exam questions and answersrahulNo ratings yet
- Final TTR Na Jud NiDocument1 pageFinal TTR Na Jud NiRene Fuentes CalunodNo ratings yet
- Edu Methods Careers GuidanceDocument8 pagesEdu Methods Careers GuidanceMs KCNo ratings yet
- B.ed SyllabusDocument123 pagesB.ed SyllabusextraworkxNo ratings yet
- Types and Conditions of Social Adaptation ExplainedDocument8 pagesTypes and Conditions of Social Adaptation ExplainedAlbina ScutaruNo ratings yet
- Values Education Website by Nonette MarteDocument12 pagesValues Education Website by Nonette MarteJoviner Yabres LactamNo ratings yet
- 02 Handout 1Document6 pages02 Handout 1Nhov CabralNo ratings yet
- Task Sheet 1.1-5 RevisedDocument3 pagesTask Sheet 1.1-5 RevisedEL FuentesNo ratings yet
- Sources For Writing An NSF CAREER ProposalDocument2 pagesSources For Writing An NSF CAREER ProposalBitao LaiNo ratings yet
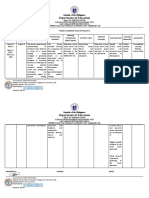
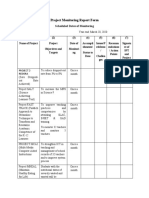
- Project Monitoring Report FormDocument3 pagesProject Monitoring Report FormAireen SiagaNo ratings yet