You might also like
- F16 Stroke Positioning ChartDocument1 pageF16 Stroke Positioning ChartSue Verge0% (1)
- Manual Muscle Testing of Infants, Toddlers Hal 4-9Document7 pagesManual Muscle Testing of Infants, Toddlers Hal 4-9deasy100% (1)
- 13 585a PDFDocument2 pages13 585a PDFtomeytto100% (1)
- Amp No ProDocument2 pagesAmp No ProHardeep Singh BaliNo ratings yet
- Fim Item ScoringDocument10 pagesFim Item Scoringhaythamalshikh0120% (1)
- Development of Multipurpose Fiber Extracting Machine FinalDocument25 pagesDevelopment of Multipurpose Fiber Extracting Machine FinalZandro A. GagoteNo ratings yet
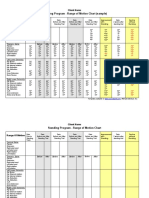
- Standing Program - Range of Motion Chart (Sample) : Client NameDocument2 pagesStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNo ratings yet
- Sitbat 16item FinalDocument6 pagesSitbat 16item FinalMae NocheNo ratings yet
- Lab PDFDocument5 pagesLab PDFNinoe CueyNo ratings yet
- Exercises For HypermobilityDocument3 pagesExercises For HypermobilityAlissa KNo ratings yet
- Upper Body Thera Band Exercise Program - BasicDocument7 pagesUpper Body Thera Band Exercise Program - Basicakheel ahammed100% (1)
- Electricity From WalkingDocument8 pagesElectricity From WalkingSanthosh100% (6)
- Blow Off Valves DescriptionDocument12 pagesBlow Off Valves DescriptionParmeshwar Nath TripathiNo ratings yet
- Monitoring Training PDFDocument264 pagesMonitoring Training PDFDiego Rojo100% (6)
- AK Bolt Gap SetupDocument22 pagesAK Bolt Gap SetupAdam Hemsley100% (2)
- CompreDocument53 pagesCompreGEr JrvillaruEl0% (3)
- MMT 6-1Document20 pagesMMT 6-1Mughal ZadiiNo ratings yet
- Self-Range of MotionDocument6 pagesSelf-Range of MotionKath100% (1)
- Orthosisofhandppt 181202162551Document65 pagesOrthosisofhandppt 181202162551Khageswar SamalNo ratings yet
- Passive MovementsDocument1 pagePassive MovementsomhreemaimhreemNo ratings yet
- Tug Test-A PDFDocument1 pageTug Test-A PDFalqurina norizkaNo ratings yet
- Upper Extremity Rom NormsDocument3 pagesUpper Extremity Rom Normsapi-336924644No ratings yet
- Assist Patient From The Bed To Chair or WheelchairDocument1 pageAssist Patient From The Bed To Chair or WheelchairKryztalGhail Llanora100% (1)
- Design of A Hand OrthosisDocument251 pagesDesign of A Hand OrthosisIsrael BlancoNo ratings yet
- Fma Ue EnglishDocument3 pagesFma Ue EnglishAnaa ElleyNo ratings yet
- MGH Wrist and Elbow Strengthening ExercisesDocument1 pageMGH Wrist and Elbow Strengthening ExercisesRidwan Hadinata SalimNo ratings yet
- Ankle & Foot Flexibility ExercisesDocument3 pagesAnkle & Foot Flexibility Exercisesnyeska100% (2)
- Proc RangeOfMotionDocument4 pagesProc RangeOfMotionSri KuspartianingsihNo ratings yet
- Cervicothoracic ExamDocument1 pageCervicothoracic ExamChristopher NotleyNo ratings yet
- Joint ROMDocument2 pagesJoint ROMdr_gentel19No ratings yet
- Exit Project Workbook Complete Draft 2Document2 pagesExit Project Workbook Complete Draft 2vladNo ratings yet
- Bubble Inclinometer Measurement Chart PDFDocument2 pagesBubble Inclinometer Measurement Chart PDFsyedqutub16No ratings yet
- Post Stroke Functional Exercises For RehabilitationDocument37 pagesPost Stroke Functional Exercises For Rehabilitationjoel_simon_23100% (1)
- Manual TherapyDocument16 pagesManual TherapylecturioNo ratings yet
- 891 Paediatric Idiopathic FlatfootDocument12 pages891 Paediatric Idiopathic FlatfootRobertus Dwi AtmokoNo ratings yet
- BKA ExercisesDocument8 pagesBKA ExercisesMary Hope A. LimaNo ratings yet
- Case History Frozen ShoulderDocument2 pagesCase History Frozen ShoulderSaliha Akram0% (1)
- Timed Up and Go Test InstructionsDocument3 pagesTimed Up and Go Test InstructionsWasemBhatNo ratings yet
- GAIT 2 - Clinical Gait Analysis - HandoutDocument32 pagesGAIT 2 - Clinical Gait Analysis - Handoutj100% (2)
- Alliance Rehab & Physical Therapy Medical HistoryDocument2 pagesAlliance Rehab & Physical Therapy Medical HistoryAlliance Physical Therapy100% (1)
- SCALE-Selective Control Assesment PDFDocument3 pagesSCALE-Selective Control Assesment PDFjinil raj j.r.No ratings yet
- Free Ebook Stroke Exercises 2022Document24 pagesFree Ebook Stroke Exercises 2022Darmawan Rizki Fauzi100% (2)
- Chapter 10 Upper Extremity Interventions PDFDocument208 pagesChapter 10 Upper Extremity Interventions PDFRonny Méndez VasconcellosNo ratings yet
- PNF For Lower LimbDocument22 pagesPNF For Lower LimbsanalcrazyNo ratings yet
- Stroke UE ToolkitDocument69 pagesStroke UE ToolkitWhitney JosephNo ratings yet
- Gait in Children With Cerebral PalsyDocument5 pagesGait in Children With Cerebral PalsyvarahamihirNo ratings yet
- Wolf Motor Function TestDocument23 pagesWolf Motor Function TestSai RamNo ratings yet
- Shoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFDocument31 pagesShoulder Guidelines AdhesiveCapsulitis JOSPT May 2013 PDFRulyNo ratings yet
- Shoulder Impingement GuidelinesDocument3 pagesShoulder Impingement GuidelinesTasha MillerNo ratings yet
- Berg Balance ScaleDocument4 pagesBerg Balance ScaleSanjanaNo ratings yet
- HEP2GO Carpal Tunnel Program PDFDocument2 pagesHEP2GO Carpal Tunnel Program PDFBetty OberackerNo ratings yet
- Spinal Cord InjuryDocument39 pagesSpinal Cord InjuryrahatNo ratings yet
- GWS Total Hip ReplacementDocument17 pagesGWS Total Hip ReplacementRadu MoglanNo ratings yet
- Normal Joint ROMDocument4 pagesNormal Joint ROMWasemBhatNo ratings yet
- Stretching Exercises For WomenDocument8 pagesStretching Exercises For Womengiriraj_mohta_1No ratings yet
- PD 8278 Energy Conservation PDFDocument4 pagesPD 8278 Energy Conservation PDFahmad kusnaeniNo ratings yet
- Suspension Therapy: DPT, Semester 2Document16 pagesSuspension Therapy: DPT, Semester 2Fatima SeharNo ratings yet
- Anterior Shoulder DislocationDocument2 pagesAnterior Shoulder DislocationcilengsaiNo ratings yet
- GRASP All 3 Levels11490 PDFDocument115 pagesGRASP All 3 Levels11490 PDFAmit ZalaNo ratings yet
- Berg Balance ScaleDocument4 pagesBerg Balance Scaletimirbpt1100% (1)
- Functional Reach TestDocument3 pagesFunctional Reach TestMarcelo Fabian Alvarado GijonNo ratings yet
- Classification of Upper Limb Orthosis: Presented To: Miss Soonhan Rani Presented By: Syeda Zoha Hassan TaqviDocument16 pagesClassification of Upper Limb Orthosis: Presented To: Miss Soonhan Rani Presented By: Syeda Zoha Hassan Taqvizoha hassanNo ratings yet
- Cardio Pulmonary AssessmentDocument8 pagesCardio Pulmonary AssessmentSHAIK SHABEENANo ratings yet
- Movement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementFrom EverandMovement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementNo ratings yet
- Exercise your way to health: Arthritis: Exercise plans to improve your lifeFrom EverandExercise your way to health: Arthritis: Exercise plans to improve your lifeNo ratings yet
- Petitioners vs. vs. Respondents Amadeo D. Seno Roderico C. VillaroyaDocument16 pagesPetitioners vs. vs. Respondents Amadeo D. Seno Roderico C. VillaroyaJAMNo ratings yet
- Module 3 Docket SystemDocument26 pagesModule 3 Docket SystemGinoong Kim GalvezNo ratings yet
- Manual Call Points: GeneralDocument2 pagesManual Call Points: GeneralAnugerahmaulidinNo ratings yet
- (WWW - Asianovel.com) - Liu Yao The Revitalization of Fuyao Sect Vol.1 Chapter 1 - Vol.1 Chapter 8Document77 pages(WWW - Asianovel.com) - Liu Yao The Revitalization of Fuyao Sect Vol.1 Chapter 1 - Vol.1 Chapter 8AnjyNo ratings yet
- Best Practices in Digital RadiographyDocument30 pagesBest Practices in Digital RadiographyJulian HutabaratNo ratings yet
- Sample High School Argumentative EssayDocument1 pageSample High School Argumentative EssayAllihannah PhillipsNo ratings yet
- Ali 2006Document7 pagesAli 2006Django BoyeeNo ratings yet
- NEET 2020 Exam Date Announced: Application, Eligibility, Dates, Admit Card, ResultDocument23 pagesNEET 2020 Exam Date Announced: Application, Eligibility, Dates, Admit Card, ResultnagaraniNo ratings yet
- Wang 2016Document7 pagesWang 2016Hadiza PebramaNo ratings yet
- 1 s2.0 S2590098621000130 MainDocument8 pages1 s2.0 S2590098621000130 MainEgo-free New-earthNo ratings yet
- Interpreting Medication OrdersDocument11 pagesInterpreting Medication Ordersmedgeek nmeNo ratings yet
- 2022 04 01 Vogue SingaporeDocument174 pages2022 04 01 Vogue SingaporeKo KoNo ratings yet
- 13 Vassileva Pediatric DRLDocument57 pages13 Vassileva Pediatric DRLLavinia BaracNo ratings yet
- Grade 7 3rd Term English Question 2078Document8 pagesGrade 7 3rd Term English Question 2078Deependra SilwalNo ratings yet
- CRSBS BrochureDocument2 pagesCRSBS BrochureKarthik PalaniswamyNo ratings yet
- University of Mumbai: (Computer Systems and ApplicationsDocument21 pagesUniversity of Mumbai: (Computer Systems and ApplicationsManish YadavNo ratings yet
- MDA Report Tata Industries FY20 21Document6 pagesMDA Report Tata Industries FY20 21Darshan VadherNo ratings yet
- FAQ Cork Fabric Folclore Crafts 2018Document7 pagesFAQ Cork Fabric Folclore Crafts 2018gabrielampNo ratings yet
- DFT Notes PDFDocument4 pagesDFT Notes PDFkrishna prasad ghantaNo ratings yet
- B-Gl-385-008 Rocket, High Explosive, 66 MM, NM 72 E5Document85 pagesB-Gl-385-008 Rocket, High Explosive, 66 MM, NM 72 E5Jared A. Lang100% (1)
- DEVICE Exp 4 StudentDocument4 pagesDEVICE Exp 4 StudentTouhid AlamNo ratings yet
- Writing A Parable (Grade 8)Document16 pagesWriting A Parable (Grade 8)JON-VIC FIGUEROANo ratings yet
- HVDC Ground ElectrodeDocument13 pagesHVDC Ground ElectrodeHeather CarterNo ratings yet
- Biodiversity in Sulawesi IslandDocument9 pagesBiodiversity in Sulawesi IslandNfdhNo ratings yet