You might also like
- Endo Test Bank 1Document6 pagesEndo Test Bank 1mildred alidon100% (1)
- NHIC PT & OT Billing and CodingDocument83 pagesNHIC PT & OT Billing and Codingsbtappouni0% (1)
- Organ DonationDocument44 pagesOrgan DonationKlause Kenze Kabil50% (2)
- Manual of Reconstructive Hand SurgeryDocument339 pagesManual of Reconstructive Hand Surgerybansai teamNo ratings yet
- Tropmed 83 690 PDFDocument6 pagesTropmed 83 690 PDFabbhyasa5206No ratings yet
- 2023 Article 378Document15 pages2023 Article 378Thaís ChouinNo ratings yet
- Laboratory Diagnostics of Dengue Fever: An Emphasis On The Role of Commercial Dengue Virus Nonstructural Protein 1 Antigen Rapid TestDocument8 pagesLaboratory Diagnostics of Dengue Fever: An Emphasis On The Role of Commercial Dengue Virus Nonstructural Protein 1 Antigen Rapid TestVijay chNo ratings yet
- Documento Con Títulos y Abstracts de Los Artículos EncontradosDocument15 pagesDocumento Con Títulos y Abstracts de Los Artículos EncontradosDaniel NietoNo ratings yet
- Dengue ICT NS1 PDFDocument7 pagesDengue ICT NS1 PDFAsti Rizki Arum PermanaNo ratings yet
- Titles and AbstractsDocument24 pagesTitles and AbstractsDaniel NietoNo ratings yet
- Sensitif Spesifik Tes DengueDocument6 pagesSensitif Spesifik Tes DengueAldy WaveNo ratings yet
- 24, Transmision en Defervescencia 2020Document5 pages24, Transmision en Defervescencia 2020Raquel FernandezNo ratings yet
- Viral GeneticDocument10 pagesViral Geneticfirdaus.kabiruNo ratings yet
- Safety and Immunogenicity of A Single Dose, Live-Attenuated Tetravalent Dengue Vaccine Feb 2022Document8 pagesSafety and Immunogenicity of A Single Dose, Live-Attenuated Tetravalent Dengue Vaccine Feb 2022Reinaldi octaNo ratings yet
- Demam Berdarah Dengue Concurrent Infections of Dengue Viruses Serotype 2 and 3 in Patient With Severe Dengue From Jakarta IndonesiaDocument7 pagesDemam Berdarah Dengue Concurrent Infections of Dengue Viruses Serotype 2 and 3 in Patient With Severe Dengue From Jakarta IndonesiaAura DiscyacittaNo ratings yet
- Biosensors and Bioelectronics: Daniel Wasik, Ashok Mulchandani, Marylynn V. YatesDocument6 pagesBiosensors and Bioelectronics: Daniel Wasik, Ashok Mulchandani, Marylynn V. YatesSamar D'melloNo ratings yet
- Deteksi Dini Virus Dengue Pada Sediaan Apus Darah Tipis Dan Tebal Dengan Metode ImunositokimiaDocument7 pagesDeteksi Dini Virus Dengue Pada Sediaan Apus Darah Tipis Dan Tebal Dengan Metode ImunositokimiaCinta Ocha KiranaNo ratings yet
- Laboratory Diagnosis For DengueDocument4 pagesLaboratory Diagnosis For DengueHamid RazaNo ratings yet
- Comparison of Diagnostic Tests For Detection of Nonstructural-1 (NS1) Antigen Dengue Virus Using Immunochromatography and Fluorescence Immunoassay MethodsDocument6 pagesComparison of Diagnostic Tests For Detection of Nonstructural-1 (NS1) Antigen Dengue Virus Using Immunochromatography and Fluorescence Immunoassay MethodsYesi ApridianaNo ratings yet
- Performance of Simplexa Dengue Molecular Assay Compared To Conventional and SYBR Green RT-PCR For Detection of Dengue Infection in IndonesiaDocument10 pagesPerformance of Simplexa Dengue Molecular Assay Compared To Conventional and SYBR Green RT-PCR For Detection of Dengue Infection in IndonesiatyaminooNo ratings yet
- Definitive Tests For Dengue Fever When and Which SDocument5 pagesDefinitive Tests For Dengue Fever When and Which SAlone EvensNo ratings yet
- SinglaDocument25 pagesSinglakasandraharahapNo ratings yet
- JJJJJJJJDocument4 pagesJJJJJJJJfreddyNo ratings yet
- Viruses 14 02073 PDFDocument17 pagesViruses 14 02073 PDFKRATIKA TYAGINo ratings yet
- Dengue InglesDocument10 pagesDengue InglesalejandroNo ratings yet
- Oral DNA Vaccines Based On CS-TPP Nanoparticles and AlginateDocument12 pagesOral DNA Vaccines Based On CS-TPP Nanoparticles and AlginateRodolfo VelazcoNo ratings yet
- Molecular Technic of Virus IdentificationDocument13 pagesMolecular Technic of Virus Identificationpratiwi kusumaNo ratings yet
- Denv MalaysiaDocument20 pagesDenv MalaysiaGabriella StefanieNo ratings yet
- 1 s2.0 S1876034119302473 MainDocument6 pages1 s2.0 S1876034119302473 MainYS NateNo ratings yet
- 08-0923 FinaldDocument5 pages08-0923 FinaldAndri YansyahNo ratings yet
- 08-0923 FinaldDocument5 pages08-0923 FinaldAndri YansyahNo ratings yet
- Wijeratne2019 PDFDocument10 pagesWijeratne2019 PDFRudy Arindra WijayaNo ratings yet
- Dengue TOT Virology, Pathogenesis Lab Diag. 2023Document44 pagesDengue TOT Virology, Pathogenesis Lab Diag. 2023ATHIBAN VNo ratings yet
- 12 ArtikelDocument8 pages12 ArtikelArrahmi Hutami HasbilaNo ratings yet
- Dengue Virus DissertationDocument7 pagesDengue Virus DissertationDoMyCollegePaperJackson100% (1)
- Vaccines 08 00063Document13 pagesVaccines 08 00063Stephany Mendez MendozaNo ratings yet
- Surgery BedahDocument5 pagesSurgery BedahHari SudrajatNo ratings yet
- 7 PDFDocument5 pages7 PDFDenny DedenNo ratings yet
- Dengue Virus ThesisDocument7 pagesDengue Virus Thesisafjvbpvce100% (1)
- 2016 Article 1849 PDFDocument8 pages2016 Article 1849 PDFdydy_7193No ratings yet
- Dokumen - Tips PPT Gagal NapaspptxDocument12 pagesDokumen - Tips PPT Gagal NapaspptxIndra Mahardhika PNo ratings yet
- 1 s2.0 S1201971221007682 MainDocument7 pages1 s2.0 S1201971221007682 MaindagbaNo ratings yet
- Vol 21 No 1 - SANTOS - Clinical Risk Score FinalDocument12 pagesVol 21 No 1 - SANTOS - Clinical Risk Score FinalAnnsh Hadji EliasNo ratings yet
- Performance Evaluation of A Dengue Iggigm and ns1 Rapid Test Device For Profesional in Vitro Diagnostic Use in Whole BloDocument3 pagesPerformance Evaluation of A Dengue Iggigm and ns1 Rapid Test Device For Profesional in Vitro Diagnostic Use in Whole BloHas SimNo ratings yet
- Kel B-10 Early Diagnosis of Dengue in Travelers PDFDocument5 pagesKel B-10 Early Diagnosis of Dengue in Travelers PDFWahyu FirmansyahNo ratings yet
- Journal - Pone.0098785 1Document9 pagesJournal - Pone.0098785 1Haradhan PalNo ratings yet
- Celgosivir Effect On DengueDocument10 pagesCelgosivir Effect On DengueKudelko MatNo ratings yet
- An Early Evaluation On The Usefulness of NS1 Antigen-Capture ELISA Versus IGM ELISA TEST For The Diagnosis of Acute Dengue InfectionDocument10 pagesAn Early Evaluation On The Usefulness of NS1 Antigen-Capture ELISA Versus IGM ELISA TEST For The Diagnosis of Acute Dengue Infectionkurniawan naryoNo ratings yet
- Dengue Hemorrhagic Fever in Infants: A Study of Clinical and Cytokine ProfilesDocument12 pagesDengue Hemorrhagic Fever in Infants: A Study of Clinical and Cytokine ProfilesYono FabiandiNo ratings yet
- H1N1 PDFDocument7 pagesH1N1 PDFanon_235643778No ratings yet
- H1N1Document7 pagesH1N1anon_235643778No ratings yet
- Infectious Diseases: Clinical Significance of Different Bacterial Load of in Patients With PneumoniaDocument5 pagesInfectious Diseases: Clinical Significance of Different Bacterial Load of in Patients With PneumoniaJaya Semara PutraNo ratings yet
- Research Paper On Dengue VirusDocument6 pagesResearch Paper On Dengue Virusfvgy6fn3100% (1)
- Journal WHODocument5 pagesJournal WHOMerina MatheosNo ratings yet
- Suppression of Virus Specific Immune Responses by IL-10 in Acute Dengue InfectionDocument10 pagesSuppression of Virus Specific Immune Responses by IL-10 in Acute Dengue InfectionThuongNguyen1981No ratings yet
- Microbiolres 08 05564Document4 pagesMicrobiolres 08 05564Prashant MishraNo ratings yet
- Hubungan Ratio Neurtofil Dan Limfosit Pada Penderita Penyakit Infeksi Virus DengueDocument7 pagesHubungan Ratio Neurtofil Dan Limfosit Pada Penderita Penyakit Infeksi Virus DengueAgusta Cahya UdayanaNo ratings yet
- Evaluation of OneStep Dengue NS1 RapiDip™ InstaTest and OneStep Dengue FeverDocument21 pagesEvaluation of OneStep Dengue NS1 RapiDip™ InstaTest and OneStep Dengue FeverSilvia PranitaNo ratings yet
- Literature Review On Dengue VirusDocument7 pagesLiterature Review On Dengue Virusaflskeqjr100% (1)
- CE7 CLIA-YHLO EBV - Clinical Characteristics of Primary and Reactivated EBV Infection in ChildrenDocument24 pagesCE7 CLIA-YHLO EBV - Clinical Characteristics of Primary and Reactivated EBV Infection in ChildrenMegdame AlnourNo ratings yet
- 16 ArtikelDocument8 pages16 ArtikelYesi ApridianaNo ratings yet
- Is New Dengue Vaccine Efficacy Data A Relief or Cause For ConcernDocument6 pagesIs New Dengue Vaccine Efficacy Data A Relief or Cause For ConcernTaufiqurrokhman RofiiNo ratings yet
- Anti-SARS-CoV-2 IgG Antibody Response Among Indian COVID-19 PatientsDocument6 pagesAnti-SARS-CoV-2 IgG Antibody Response Among Indian COVID-19 PatientsdhairyasheelNo ratings yet
- Management of Infections in the Immunocompromised HostFrom EverandManagement of Infections in the Immunocompromised HostBrahm H. SegalNo ratings yet
- GINA 2019 Main Pocket Guide Wms PDFDocument39 pagesGINA 2019 Main Pocket Guide Wms PDFmyikellaNo ratings yet
- Laporan MRIN GenomicDocument18 pagesLaporan MRIN Genomiccindy clarissaNo ratings yet
- The Effect of Exercise On Blood Pressure and Heart RateDocument1 pageThe Effect of Exercise On Blood Pressure and Heart Ratecindy clarissaNo ratings yet
- Laporan MRIN GenomicDocument18 pagesLaporan MRIN Genomiccindy clarissaNo ratings yet
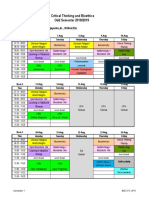
- Critical Thinking and Bioethics Odd Semester 2018/2019: Block Coordinator: Rhendy Wijayanto, DR., M.Med - EdDocument2 pagesCritical Thinking and Bioethics Odd Semester 2018/2019: Block Coordinator: Rhendy Wijayanto, DR., M.Med - Edcindy clarissaNo ratings yet
- Critical Thinking and Bioethics Odd Semester 2018/2019: Block Coordinator: Rhendy Wijayanto, DR., M.Med - EdDocument2 pagesCritical Thinking and Bioethics Odd Semester 2018/2019: Block Coordinator: Rhendy Wijayanto, DR., M.Med - Edcindy clarissaNo ratings yet
- Kisi2 BiochemDocument4 pagesKisi2 Biochemcindy clarissaNo ratings yet
- Kisi2 BiochemDocument4 pagesKisi2 Biochemcindy clarissaNo ratings yet
- A Migraine Headache PresentationDocument14 pagesA Migraine Headache PresentationAbdullah Masud TanjimNo ratings yet
- DuchenneDocument13 pagesDuchennejenika studiesNo ratings yet
- Laporan RPUDocument9 pagesLaporan RPUddeeppeeNo ratings yet
- Tingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulDocument6 pagesTingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulRusnaneeNo ratings yet
- Your Guide To Post Surgery Care - Major - CleanDocument28 pagesYour Guide To Post Surgery Care - Major - CleanZar Chi LinNo ratings yet
- Loresca - Ratio Mtle - HistopathDocument10 pagesLoresca - Ratio Mtle - HistopathKaycee Gretz LorescaNo ratings yet
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- Glaukoma - PPTX KoassDocument38 pagesGlaukoma - PPTX Koassdhita01No ratings yet
- SO PER TGL 07 MEI 2021 Material Medika PlazaDocument56 pagesSO PER TGL 07 MEI 2021 Material Medika PlazaWìwHi TawvhiNo ratings yet
- Scalp Acupuncture Treatment Protocol For Anxiety Disorders: A Case ReportDocument6 pagesScalp Acupuncture Treatment Protocol For Anxiety Disorders: A Case ReportTanuku NetNo ratings yet
- Spinal Cord InjuryDocument28 pagesSpinal Cord InjuryLouie John AbilaNo ratings yet
- Most Common Chronic Pain ConditionsDocument7 pagesMost Common Chronic Pain ConditionsNicolas RitoNo ratings yet
- C. Pasternatsky Symptom IsDocument11 pagesC. Pasternatsky Symptom IsareenNo ratings yet
- Iem India Perspective N B Kumta MaharashtraDocument8 pagesIem India Perspective N B Kumta Maharashtraavijitcu2007No ratings yet
- Bipolar 1 Disorder NCPDocument3 pagesBipolar 1 Disorder NCPJoy-Rena Sabinay OchondraNo ratings yet
- Demodex Infestation Requires Immediate, Aggressive Treatment by Doctor, Patient - Primary Care Optometry NewsDocument5 pagesDemodex Infestation Requires Immediate, Aggressive Treatment by Doctor, Patient - Primary Care Optometry NewsΔιονύσης ΦιοραβάντεςNo ratings yet
- Threshold and RecruitmentDocument16 pagesThreshold and RecruitmentShamaine Anne SalvadorNo ratings yet
- Hcs Customer BrochureDocument43 pagesHcs Customer BrochureKunalNo ratings yet
- Morning Report Obs FebrisDocument10 pagesMorning Report Obs FebrisJessicaNo ratings yet
- Maxillofacial - Infection - Dari KikiDrDocument20 pagesMaxillofacial - Infection - Dari KikiDrmashitadyahNo ratings yet
- Effectiveness of Structured Teaching Program On Self-Medication Knowledge and Its Adverse Effects Among Middle Age Adults Residing in Lalitpur, NepalDocument8 pagesEffectiveness of Structured Teaching Program On Self-Medication Knowledge and Its Adverse Effects Among Middle Age Adults Residing in Lalitpur, NepalIJAR JOURNALNo ratings yet
- A Three-Dimensional Method of Visualizing The Temporomandibular Joint Based On Magnetic Resonance Imaging in A Case of Juvenile Chronic ArthritisDocument7 pagesA Three-Dimensional Method of Visualizing The Temporomandibular Joint Based On Magnetic Resonance Imaging in A Case of Juvenile Chronic ArthritisNAGARAJNo ratings yet
- Important Notice - 59 - 2022 Dated 22.03.2022 Available Seats Foreign National Spon INI CET PG Courses July 2022Document2 pagesImportant Notice - 59 - 2022 Dated 22.03.2022 Available Seats Foreign National Spon INI CET PG Courses July 2022Bilal Ahmed MultaniNo ratings yet
- Rotator Cuff Tears: Review of Epidemiology, Clinical Assessment and Operative TreatmentDocument15 pagesRotator Cuff Tears: Review of Epidemiology, Clinical Assessment and Operative Treatmentsm - kardmNo ratings yet
- Description of The Strategy: Feedback Is A Process in Which The Factors That Produce A Result Are Themselves ModifiedDocument8 pagesDescription of The Strategy: Feedback Is A Process in Which The Factors That Produce A Result Are Themselves Modifiediulia9gavrisNo ratings yet
- Glossary and Acronyms of FreedivingDocument2 pagesGlossary and Acronyms of FreedivingIvo XNo ratings yet